
In recent years, there has been a growing debate about what role foundations should play in global health governance generally, and particularly vis-a-vis the World Health Organization (WHO). Much of this discussion revolves around today’s gargantuan philanthropy, the Bill and Melinda Gates Foundation, and its sway over the agenda and modus operandi of global health. Yet such pre-occupations are not new. The Rockefeller Foundation (RF), the unparalleled 20th century health philanthropy heavyweight, both profoundly shaped WHO and maintained long and complex relations with it, even as both institutions changed over time
Backstage: the relationship between the Rockefeller Foundation and the World Health Organization, Part I: 1940-1960s by A.-E. Birn – 2013 The Royal Society for Public Health
According to the Rockefeller Foundation official website, John D. Rockefeller Sr.’s interest in health was in large part influenced by Frederick T. Gates, who was Rockefeller’s philanthropic advisor. Gates had a personal interest in medical research, and he believed strongly that it could be of universal benefit. In 1901, Gates persuaded Rockefeller to fund the creation of the Rockefeller Institute of Medical Research (RIMR) to research the causes, prevention and cures of disease. While financial support for the RIMR was initially disbursed in small increments, by 1928 the organization had received $65 million in Rockefeller funding.
Born in 1853 to a Baptist minister, Gates was raised with a strong dedication to his faith. After graduating from the University of Rochester in New York in 1877 and the Rochester Theological Seminary in 1880, he was ordained as a Baptist minister and spent the next eight years as pastor of the Central Baptist Church in Minneapolis, Minnesota.
In 1888 while working as Secretary for the American Baptist Education Society, Gates came to the attention of John D. Rockefeller (JDR). JDR was approached by Gates as part of a campaign to create a major Baptist university in the Midwest. Convinced by Gates’ arguments for such an institution, JDR became the principal benefactor of what became the University of Chicago in 1892.
JDR was impressed by Gates’ fundraising and planning skills and proposed that Gates come to manage his philanthropic and business activities.
From this position Gates established his legacy in the field of philanthropy. In 1897, inspired by the lack of medical research facilities in the U.S., Gates laid out a plan for opening an American medical research institution. This plan – his first major endeavor as Rockefeller’s philanthropic advisor – led to the creation of the Rockefeller Institute for Medical Research. He also played an essential role in creating and organizing the General Education Board (GEB) in 1902 and the Rockefeller Sanitary Commission (RSC) for the Eradication of Hookworm Disease in 1909.
His most notable contribution to early philanthropy, however, was his role in the establishment of the Rockefeller Foundation (RF). It was Gates’ vision of a large, professionally staffed foundation that could work for the general purpose of “the welfare of mankind” that convinced JDR to provide the resources for the new foundation. During his time on the RF Board of Trustees, Gates encouraged a focus on health initiatives (setting an agenda that prevailed for decades) and oversaw early activities of the Foundation, including the development of the International Health Division (IHD) and the China Medical Board (CMB). He served a ten-year term on the RF Board of Trustees before retiring in 1923.
Any lawsuit against the Rockefeller Foundation is a lawsuit against the ones who funded not only Mengele’s, but all the others’ grotesque Auschwitz experiments and are behind serious threats to humanity in the present.
– Exopolitics
Rockefellers funded the Nazi experiments in the concentrations camps
Jews who know the history of WWII are aware that it was IG Farben, the pharmaceutical and chemical giant, which put Hitler into office and ran the camps. And they know that the Rockefellers had half interest in IG Farben and IG Farben had half interest in the Rockefellers’ Standard Oil.
But while they know that Auschwitz was the site of hideous forced human “medical experiments,” most Jews believe that the horrors of Nazi experiments ended in Nazi Germany.
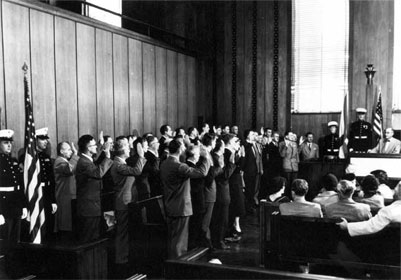
Rockefellers brought the Nazi doctors and researchers to the US
The Rockefellers and OSS (now the CIA) brought Nazi “doctors” and “researchers” to the US under a program called Operation Paperclip. Nazis were given new identities, false passports, and inserted into medical institutions, and bioweapons, aerospace, military, and spy agencies here, and also were helped to escape to and do similar work for other countries and global agencies. There is reason to believe based on the actions of those global agencies, that some also became part of the newly established UN – including WHO, UNICEF, and UNESCO.
CIA’s Denial of Protecting Nazis is Blatant Lie
by Hank P. Albarelli Jr.
VOLTAIRE NETWORK | 7 DECEMBER 2010
Leaks or revelations are often more compelling because of what they don’t reveal. Through Operation Paperclip, the U.S. organized a monumental transfer of black technology by actively recruiting Nazi criminals for employment by U.S. intelligence. Author H. P. Albarelli excavates the part that was missing from the recently-outed official report: the U.S. pointedly chose fervent Nazi scientists with experience in chemical, biological and radioactive warfare to become the architects of the CIA’s darkest military experiments with human guinea pigs, reminiscent of Nazi Germany.
Marvin Washington Brooks had been terribly ill for nearly three months.
A year prior in early-1952, he had been diagnosed with cancer and had been admitted as “a patient for treatment” to the University of Texas Medical School’s M.D. Anderson Hospital. Brooks had served as an infantryman in the Army during World War II. He had received a Purple Heart for being wounded during the Battle of the Bulge. Not long after he was admitted to the M.D. Anderson Hospital, Brooks began to receive weekly treatment from a team of physicians led by an older doctor with a heavy German accent and three distinctive scars across his face. Brooks was told the treatment could significantly affect his cancer in positive ways. But Brooks had become increasingly ill, with constant vomiting, weight and hair loss, and patchy skin with large areas appearing as if severely sunburned. Within about six months of the weekly treatment, Brooks was in constant pain. He died the first month of 1955, two days before what would have turned 47 years old. Brooks was never informed that he was one of 263 cancer patients who were secretly being experimented upon with “whole body irradiation.” Brooks, nor his wife or family, had ever been consulted about the experiments. Nor had Brooks, or anyone else, given the hospital permission to experiment on him. Nobody ever told Brooks, or anyone in his family, that the German physician who saw him weekly was Dr. Herbert Bruno Gerstner, a former Nazi doctor who had been secretly brought to the United States in 1949.
On November 17, 2010 the CIA’s Director of Public Affairs, George Little, wrote a short letter to the editor of the New York Times. Little, on behalf of the agency, protested a just published Times article that detailed CIA “interactions with former Nazi officials in the early years of the post World War II era.” Mr. Little wrote, “We would like to make clear that the agency at no time had a policy or a program to protect Nazi war criminals, or to help them escape justice for their actions during the war.”
The article provoking the CIA’s ire had appeared on the front page of the Times’ Sunday, November 14 edition. Written by reporter Eric Lichtblau, it was entitled “Nazi’s Were Given ’Safe Haven’ in U.S., Report Says”. The article focused on a 600-page “secret report” that had been produced by the U.S. Justice Department. The report, which Justice Department officials had suppressed from public release for years, details the American government’s importation into the U.S., following the end of World War II, of countless numbers of Nazis.
Written in a dry, bureaucratic style, the report recounts a number of examples of well-known Nazis to whom both the CIA and Department of State had provided both shelter and employment to, including Adolph Eichman, Otto Von Bolschwing, Dr. Josef Mengele, and Arthur Rudolph. To the purposes of this article, it is important to underscore here that the long-concealed report makes no mention whatsoever of the many Nazi scientists who specialized in chemical, biological and radioactive warfare and who were secretly relocated in the United States between the years 1946 and 1958.
For many readers, especially those unfamiliar with Project Paperclip, the New York Times article was stunning news. For those who were knowledgeable of the Pentagon’s and CIA’s long-overlooked aggressive efforts at recruiting and utilizing Nazi scientists the article was mostly old news, but its publication along with its accusatory finger pointing at the intelligence agency was encouraging.
While the intent here is not to cast aspersions on Mr. Little— who most likely has little knowledge about the subject in question, and was only issuing protestations at the behest of someone well above him, perhaps DCI Leon Panetta— it is to take strong exception with the CIA’s denial, and to offer ample evidence, taken from the agency’s own files among other government resources, that the denial is blatantly erroneous.

Henry Kissinger, “Rockefeller’s best employee”, the Jew that brought Nazi murderers to the US
Kissinger And Rockefeller: Connections To The CIA And The Origins Of AIDS And Ebola
The following article was written in 1996 by Dr. Leonard G. Horowitz
Six years ago [i.e. 1990], most of you can recall, the highly publicized case of the Florida dentist who infected his patients with AIDS — the case of, the beautiful teenager, Kimberly Bergalis, who died shortly after testifying before Congress in a wheel chair. At the time I was serving as the chief professional advisor to the largest dental and medical catalog supply company in the world.
The day the story broke I was assigned to develop patient and professional Educational materials to help allay the public’s growing fear of visiting dental and medical offices in the age of AIDS.
You may recall how terrified most people became about a routine trip to the dentist at that time. So I began by investigating the Centers for Disease Control and prevention’s (CDCs) official investigation reports on the case. And to make a long story short, I found the reports to be scientifically bogus.

Henry Kissinger and Nelson Rockefeller, January 1975
I later learned that the government had covered-up key evidence in the tragedy in an effort the maintain the case an Unsolvable mystery.
In essence they had committed scientific fraud and misconduct and, in the process, concealed the most incriminating evidence against the dentist — a very bright, scientifically trained, ex-military dentist, who believed he was dying of a virus that the government had created.
Yes, you heard me correctly, a virus that the government had created.
Now, the problem I had was reconciling the fact that the dentist, though a psychopath, was no fool. And he held in his possession one of the most incriminating documents I had ever seen. A 1970 Department of Defense Appropriations request for $10 million for the development of immune system ravaging Viruses for germ warfare.
In fact, the document, which I lay before you today, reads like this: Within the next 5 to 10 years, it would probably be possible to make a new infective microorganism which could differ in certain important aspects from any known disease-causing organisms.
Most important of these is that it might be refractory to the immunological and therapeutic processes upon which we depend to maintain our relative freedom from infectious disease… A research program to explore the feasibility of this could be completed in approximately 5 years at a total cost of $10 million… It is a highly controversial issue and there are many who believe such research should not be undertaken lest it lead to yet another method of massive killing of large populations.”
In fact it was the National Academy of Sciences-National Research Council (NAS-NRC) that had informed the Defense Department that this research was possible. Now, according to legal testimony given to government officials, this knowledge enraged the Florida dentist so much it moved him to intentionally inject his patients with HIV-tainted anesthetics.
In essence, he did what all organized serial killers love to do, express a vendetta, like the mail-bomber, play games with the authorities, trap them in a catch-22, whereby they’d be damned if they told the truth, and called him a serial killer, because the whole world would want to know motive, and every reporter would ultimately find out as I did, what drove him crazy and who he really hated and ultimately attacked.
And if they told a lie, or maintained the case, as they did, a mystery, it would hold America and all of health care hostage to irrational fear of routine health care in the age of AIDS.
Now all of this I documented in three published scientific reports and my last book “Deadly Innocence: The Kimberly Bergalis Case — Solving the Greatest Murder Mystery in the History of American Medicine.”
I present these publications and documents here for your critical examination. So Dr. Acer created a crime, a mystery, that couldn’t be solved, without implicating the government and causing a larger mystery to be investigated.
That is, the origin of AIDS and Ebola — the subject of my last three years of research, and why I have come before you today.
In fact, I investigated the Department of Defense’s germ warfare appropriations request and learned that the option to develop synthetic biological agents — bioweapons as alternatives to nuclear weapons — came from Dr. Henry Kissinger, who was gradually placed in his position of authority as National Security Advisor under Richard Nixon, the most powerful man in government, by Nelson Rockefeller and his affiliates at the Council on Foreign Relations.
Moreover, I traced where the money went. It went, in fact, to a firm called Litton Bionetics, a subsidiary of the mega-military contractor Litton Industries, whose President, Roy Ash, was being considered as an alternate to Henry Kissinger for the National Security Advisor post.
Instead, Roy Ash became Richard Nixon’s chairman of the Presidents Advisory Council on Executive Organizations, and Assistant to the President of the United States.
And Litton Industries was given over $5 billion in military contracts during the first term of the Nixon administration, $10 million of which went towards the development of AIDS-like viruses. A mere drop in the bucket. But before I tell you exactly what was done with your $10 million of taxpayer money, some background on Kissinger and Rockefeller’s influence is in order.
Among Henry Kissinger’s most influential patrons as he worked his way up the ladder of success to become Nixon’s Deputy to the President for National Security, was Nelson Aldrich Rockefeller, the son of Standard Oil, that is Exxon, heir John D. Rockefeller, Jr.
The Rockefeller families involvement in the medical-industrial complex, health science research, and American politics is clearly important. Before World War II, major administration of medical research, or financing by federal agencies, had been generally opposed by Americas scientific community.
In fact, it was only during times of war that organizations like the NAS or the NRC received major funding. Both the NAS, established during the Civil War, and the NRC, set up during the First World War, were largely ignored in times of peace. Between 1900 and 1940, private foundations and universities financed most medical research.
According to Paul Starr, author of The Social Transformation of American Medicine: The rise of a sovereign profession and the making of a vast industry, the most richly endowed research center, the Rockefeller Institute for Medical Research was established in New York in 1902 and by 1928 had received from John D. Rockefeller $65 million in endowment funds.
In contrast, as late as 1938, as little as $2.8 million in federal funding was budgeted for the entire U.S. Public Health Service.
Therefore, it is easy to see that Rockefeller family investment in health science research predated, and far surpassed, even the federal governments. More than the New Deal, the Second World War created the greatest boom in federal government and private industry support for medical research. Prior to the war, American science and medicine was heavily influenced by German models.
This precedent was bolstered during the 1930s when the Nazis purged Jewish scientists from German universities and biological laboratories. These changes, according to Starr, significantly altered the course of American health science and medicine.
Many of Germany’s most brilliant Jewish researchers immigrated to the United States just as the movement burgeoned to privatize war related biological and medical research. At this time, the Rockefeller led medical-industrial complex was fully poised to influence, and take advantage of, Congress first series of measures to promote cancer research and cancer control.
In 1937, the new federal legislation authorized the establishment of the National Cancer Institute under the National Institutes of Health, and, for the first time, the Public Health Service to make grants to outside researchers.
The Rockefellers exercised significant control over the outcomes of these grants and research efforts through the foundations they established. Following the war, Henry Kissinger, who had become General Alexander Bolling’s German translator and principle assistant.
(Bolling, of course, was the Godfather to the Joint Intelligence Objectives Agency that ran “Project Paperclip,” the secret exfiltration of approximately 2,000 high level Nazis, about 900 of whom were military scientists and medical researchers, including Erich Traub, Hitler’s top biological weapons developer and virus expert. Bolling also served as a high ranking member of the Inter-American Defense Board, a Washington based group that delivered Walter Emil Schreiber, Hitler’s chief medical scientist, the “Angel of Death” Joseph Mengele, and his assistant, “the butcher of Lyon,” Klaus Barbie, among others, to safe Havens in South America where they worked on CIA projects.)
In fact it was Henry Kissinger’s job to seek and find such Nazis that might be of service to America, and Kissinger became the chief of Army Counter-Intelligence in this regard. He trained other agents to hunt down Nazis at the European Command Intelligence School in Oberammergau, not to be tried for war crimes necessarily, but rather to serve U.S. military rather than Russian interests.
It was this operation that principally spirited the creation of the CIA as a cover agency for the powerful Gehlen Org, the German intelligence agency run by Reinhard Gehlen — an organization whose power superseded even the Nazi SS because of its prewar connections with German military intelligence.
After Hitler, Gehlen served Allen Welsh Dulles, whose “Operation Sunshine” brought Nazis into the U.S. spy service. You may be interested to know who paid for the importation of Nazis into American central intelligence, the military, and industry?
Three groups:
1. The first was “The Sovereign Military Order of Malta” (SMOM), perhaps the most powerful reactionary segment of European aristocracy, that for almost a thousand years, starting with the crusades in the Twelfth Century, funded military operations against countries and ideas considered a threat to its power
2. Second was the Nazi war chest that was largely funneled through the Vatican and the Rockefeller owned Chase Manhattan Bank, whose Paris branch conducted business as usual throughout the Nazi occupation of France
3. Thirdly, some of us and our parents — American taxpayers. Moreover, during this period, the Council on Foreign Relations, along with the CIA, grew in power under the leadership of Nelson Rockefeller, and in 1955, while serving as President Eisenhower’s assistant for international affairs, Rockefeller invited Kissinger to discuss national security issues at the Quantico (Virginia) Marine Base
Following their meeting, according to Walter Isaacson’s biography of Kissinger, the diplomat became Rockefeller’s closest intellectual associate, and soon after, Kissinger authored several military proposals for Eisenhower to consider. Unimpressed, Eisenhower turned them down.
As a result, Rockefeller sent Eisenhower his resignation and then launched a Special Studies Project that explored the critical choices America faced militarily in the coming years. Kissinger agreed to direct this new project and published a 468-page book on his findings.
The treatise proposed that tactical nuclear weapons be developed and a bomb shelter [be built] in every house in preparation for limited thermonuclear war. The willingness to engage in nuclear war when necessary is part of the price of our freedom, Kissinger argued.
So those of you my age can recall the anxiety grade school students felt while drilling for possible nuclear attacks. You can thank Kissinger and the Rockefeller-led military industrialists for this “price for freedom.”
Eisenhower, you may remember, warned America that the gravest threat to world security, democracy, and even spirituality, was the growing military-industrial complex. And the Rockefellers and Kissinger played leading roles in its evil expansion.
Bent on creating what President Bush openly heralded as a “New World Order,” few people realize the current international alignment of economic powers is a direct result of actualizing Henry Kissinger’s contemporary manifesto tribute to the Sovereign Military Order of Malta entitled “The Meaning of History.”
In this Kissinger 1955 Harvard doctoral thesis he argues that the concept of peace on earth is naive. Peace must be secured by the creation of small wars around the planet on a continuing basis so as to maintain an international order of economic powers, and of course, keep the military industrialists happy.
In my latest book, “Emerging Viruses: AIDS and Ebola — Nature, Accident, or Intentional?”, I traced Dr. Erich Traub’s movements to the U.S. Naval Medical Research Institute, where he conducted experiments on animals to determine the lethal doses of more than forty strains of highly infectious viruses.
Within ten years, the Navy’s Biomedical Research Laboratory, in association with the University of California, along with Litton Bionetics, became a chief supplier of viruses and cell cultures for NCI researchers throughout the world.
Funding for this work was largely controlled by the NCI, Rockefeller and Sloan Foundations. A search through Sloan Foundation’s annual reports, on file in Manhattans New York Public Library, revealed nine ghastly and Incriminating reasons that, most incredibly, tied all the elements of my “Emerging Viruses” investigation together.
The Sloan Foundation:
1. supported black educational initiatives consistent with the COINTELPRO Black Nationalist Hate Group campaign (you may recall reports last year that in surveys of 1,000 Southern Christian African Americans, two-thirds reported their belief that the AIDS epidemic may be genocide, while one-third was convinced it was
2. the Sloan Foundation administered mass-media-public-persuasion experiments completely consistent with the CIA’s Project MKULTRA efforts to develop brainwashing technologies and drugs to affect large populations
3. funded much of the earliest cancer research involving the genetic engineering of mutant viruses
4. began major funding of the National Academy of Sciences, Cold Spring Harbor Laboratory (for neuroscience and molecular genetics research), the Salk Institute (for viral research), and the Scientists Institute for Public Information between 1968 and 1970
5. funded population control studies by Planned Parenthood-World Population, New York, N.Y.
6. funded the Community Blood Council of Greater New York, Inc., the council of doctors who established the infamous New York City Blood Bank which allowed more than 10,000 hemophiliacs and countless others to become infected with HIV because they allegedly didn’t want to spend $150 million to screen the blood
7. maintained Laurence S. Rockefeller, the director of the Community Blood Council of Greater New York the international blood bankers and the president of the Rockefeller Brothers Fund, as chairman of the board of the Memorial Sloan-Kettering Cancer Center, and a trustee for the Sloan Foundation
8. gave in excess of $20,000 annually to the Council on Foreign Relations
9. maintained among its marketable securities, 16,505 shares of Chase Manhattan Bank stock (in 1967, which it apparently sold by 1970 probably to avoid conflict of interest charges) along with 24,400-53,000 shares issued by Merck & Co., Inc. (the company whose President, George W. Merck, was director of America’s biological weapons industry, and whose hepatitis B and polio jabs most plausibly transmitted AIDS throughout the world)
Also in “Emerging Viruses: AIDS and Ebola,” you will learn exactly what was done with the $10 million Congress gave the DOD for the development of AIDS-like viruses, because I published the relevant contracts.
You will learn that Dr. Robert Gallo, the famous NCI molecular biologist, pardoned by President Clinton last year for scientific fraud and misconduct, and credited with the discovery of the AIDS virus, set about to develop immune system ravaging, AIDS-like viruses, along with other Litton Bionetics researchers.
You will learn that they took monkey viruses that were humanly benign, recombined them with DNA, RNA, and enzymes from other animal viruses that caused leukemias, lymphomas, and sarcomas, and then to get them to jump species, they cultured these new mutant viruses in human white blood cells in some studies, and human fetal tissue cells in other studies, to produce immune-system-destroying, cancer-causing viruses that could enter humans and produce virtually identical effects to what the AIDS virus is currently doing in people around the world.
Indeed, it was contaminated live viral jabs that spread this disease and likely others, including chronic fatigue, certain leukemias, and possibly Gulf War Syndrome as well, to vast populations.
In fact, today’s live viral jabs, including the oral polio jab required by law be given to our children, are still littered with simian (monkey) virus contaminants since they are developed in monkey kidney cells, and the U.S. Food and Drug Administration turns a blind eye to as many as 100 live monkey virus contaminants per jab dose, and is barred from telling health professionals and even health scientists this truth because of pharmaceutical industry dictated proprietary laws and non-disclosure agreements.
In the end, the research question I asked,
“Did these viruses, AIDS and Ebola, evolve naturally, were they accidentally produced, or were they intentionally created and deployed?”
I conclude, unquestionably, they are not natural. I leave you the reader, and concerned citizens of America and the world, to decide whether it was a horrible accident or treacherous covert population control experiment.
I ask all of you to consider the pain and cost of the current and coming plagues, including the escalating rates of virus-linked cancers like prostate and breast cancer, certain leukemia’s and lymphomas and other jab contaminant related illnesses including hyperactivity disorders in children and escalating sudden infant death rates.
I believe you will realize that the pain and cost of denial and indifference to this horrible reality is far greater than the toll your political action might cost. I therefore urge you to join our growing grassroots network of health consumers, professionals, scientists, patriots, and concerned citizens in our search for answers and solutions.
I urge you to help us pressure Congress for a full investigation of these published facts, and to allocate the funding needed to effect appropriate solutions to these urgent health care problems. Let me end by giving you, and our home viewers, two resources to contact in this effort.
“Jacobsen opens Operation Paperclip in November 1944, …. two American bacteriology experts pore over a cache of documents in the apartment of Dr. Eugene Haagen, a German virus expert. Within hours they find a chilling letter from Haagen to a colleague:
“Of the 100 prisoners you sent me, 18 died in transport. Only 12 are in a condition suitable for my experiments. I therefore request that you send me another 100 prisoners between 20 and 40 years of age … .”
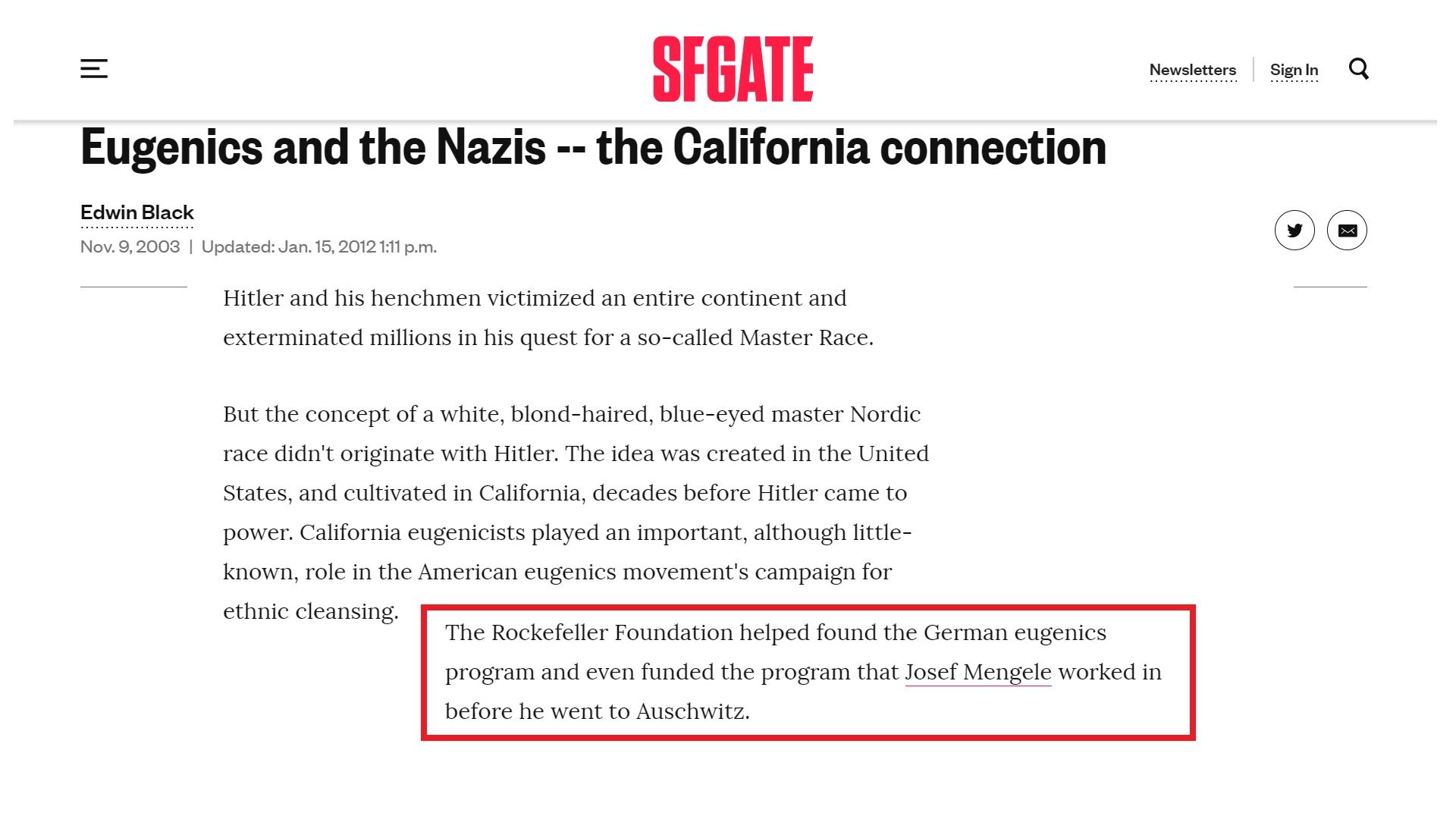
“The letter proved that the Nazis were bent on creating biological weapons for use in warfare ….”The people carrying out this barbaric work were no minor Nazi thugs: Before the war, Haagen held a fellowship with the Rockefeller Foundation ….
From: Book Review: Operation paperclip: The Secret Intelligence Program To Bring Nazi Scientists To America By Annie Jacobsen. See below book presentation by its author
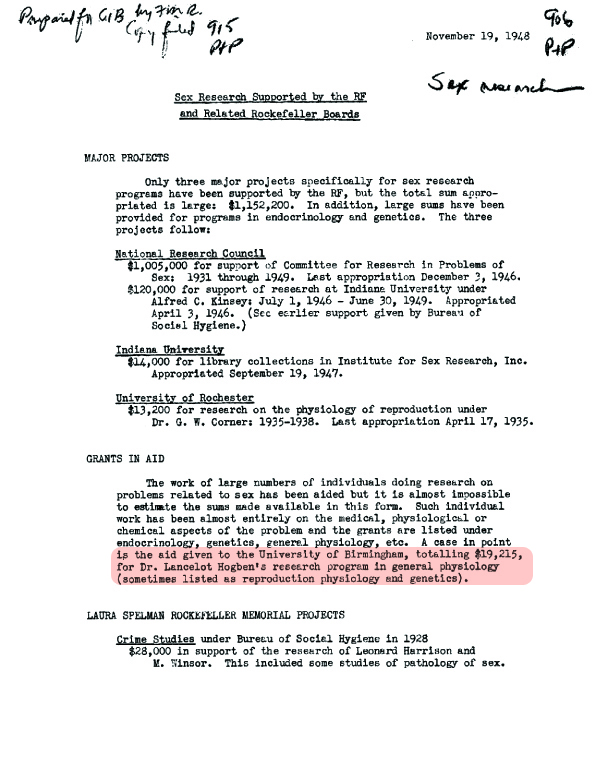
A document I’ve just dug out from the RF archives shows that around the time they were salvaging Hitler’s scientists through Operation Paperclip, the Rockefellers were already deeply involved in eugenics, genetics, human reproduction too. For the near future I’m considering an article on this topic only.
How Rockefeller Foundation Shaped Modern Medicine in Communist China
This chapter comes in RF’s own words, it’s no secret, most of the truth is not hidden, it’s people running from it:
The China Medical Board (CMB) was created in 1914 as one of the first operating divisions of the Rockefeller Foundation (RF). Provided with a $12 million endowment and separately incorporated as CMB, Inc. when the Foundation was reorganized in 1928, the Board’s aim was to modernize medical education and to improve the practice of medicine in China.
Doctors graduating from Peking Union Medical College, Beijing (China), 1947
Surveying China
China was a long-standing interest of both John D. Rockefeller, Sr. (JDR Sr.), and his son. For decades they and their fellow Baptists had supported missionary work in Asia. Beginning in the early 1900s, Frederick Gates encouraged them to devote even more attention to that region. In 1908, five years before the Foundation was created, the Rockefellers funded a commission headed by Edward D. Burton, a University of Chicago professor of theology. He and other educators traveled to China to explore the potential for philanthropic work there.
In its final report the Burton Commission argued that a Western-sponsored educational program in science and medicine for elite Chinese students could succeed, despite a difficult political climate. One of the first actions of the newly created RF was to organize a conference about China in New York in early 1914. The Foundation later dispatched two additional survey groups, the China Medical Commissions of 1914 and 1915, to gather more information about how such an educational program could operate.
Following the model established by Abraham Flexner’s survey of U.S. medical education, the 1914 Commission set out to appraise medical education in both missionary and Chinese schools. It found appallingly low standards throughout the country. The report concluded that “the country is so vast, and the resources available for dealing with the problem are so limited as yet, that the need of outside assistance is still very great.” The CMB was formed to meet those challenges, and Wallace Buttrick was named its first director.
The Foundation’s approach to Chinese medical education would inevitably follow the general patterns for reforming U.S. medical education advocated in the 1910 Flexner report and most fully embodied in the Johns Hopkins University School of Medicine. Medical education in China would be scientifically rigorous and adhere to Western standards. And, in a decision with long-term consequences, instruction would occur in English. Consequently, the school could reach only a small, elite percentage of the population. Yet in a country of 400 million people then served by fewer than 500 well-trained doctors, such an approach stood to be criticized. Nevertheless, the CMB set out to build a medical school in China that it hoped to make the equal of Johns Hopkins.
The RF entered China with an ambitious goal: to build modern medical schools in both Peking and Shanghai. By purchasing the Union Medical College from the London Missionary Society in 1915, the Foundation took its first steps toward that goal. Over the next six years the Foundation assembled a faculty of fifty professors and upgraded and enlarged the facilities of what was soon called the Peking Union Medical College (PUMC). Particular attention was paid to the school’s architecture and campus plan. According to the RF’s 1917 Annual Report, “While the buildings will embody all the approved features of a modern medical center, the external forms have been planned in harmony with the best tradition of Chinese architecture. Thus they symbolize the purpose to make the College not something foreign to China’s best ideals and aspirations, but an organism which will become part of a developing Chinese civilization.”
PUMC opened its doors in 1919, under the de facto directorship of Roger S. Greene, resident director of CMB. The 70-acre campus would ultimately encompass more than 50 buildings, including a hospital, classrooms, laboratories, and residences. But in New York Rockefeller officials grew concerned about the mounting costs of PUMC and were soon forced to scrap their plans for Shanghai. From an initial construction estimate of $1 million in 1915, expenses ballooned to $8 million in capital expenditures by 1921. The operating budget more than doubled between its first year of operation and 1921. Nevertheless, the medical school and its new campus were deemed worth celebrating. John D. Rockefeller, Jr. (JDR Jr.) led an impressive delegation to China for the 1921 dedication ceremonies.
PUMC’s initial contributions toward the improvement of medicine in China, though consequential, were inevitably limited in scale. Its graduating classes were small, in part because its standards remained high and its curriculum at the outset was exclusively in English. Between 1924 and 1943, PUMC produced only 313 doctors, more than half of whom would continue their studies abroad through CMB fellowships. Upon their return many of these doctors ultimately became leaders in medical administration, teaching and scientific research both before and after the Chinese Revolution.
PUMC also transformed the nursing profession in China. When PUMC opened, there were fewer than 300 trained nurses in the country, many of them affiliated with various missionary organizations and most of them male. Because the Chinese had never considered nursing to be an appropriate profession for women, the task of PUMC was both to train qualified women nurses and to elevate the status of the profession. Those responsibilities fell to a twenty-eight-year-old nurse from Johns Hopkins, Anna D. Wolf. She arrived in 1919 to create a training program for nurses and to organize the hospital’s nursing staff. Recruiting her initial faculty from the best U.S. nursing schools, she devised pre-nursing and nursing curricula. Within five years she established a school capable of meeting U.S. accrediting standards.
John Grant, a professor of public health at PUMC from 1921 to 1934, sought to offer medical services beyond the campus walls. He collaborated with the city’s police in 1925 to create a public health station serving the 100,000 people living in Peking’s first ward, the neighborhood surrounding PUMC. As Grant knew, the station also provided learning opportunities for students at the university. He persuaded his faculty colleagues that PUMC students should spend a four-week rotation there.
Grant’s interest in pursuing broader public health work in rural areas found responsive allies in New York. Selskar Gunn, who had worked with the International Health Division in Eastern Europe before joining RF’s Division of the Social Sciences, traveled to China in 1931 to assess the Foundation’s work. While there he met Yan Yangchu (known to his American associates as Jimmy Yen), a pioneer in mass education and leader of the Rural Reconstruction Movement, with which Grant was already working. After several trips to China, Gunn produced a report that envisioned a coordinated program of basic education, health, and economic development.
Gunn was critical of PUMC and of RF’s and CMB’s disproportionate investment in it. By 1933 almost $37 million had been spent on an institution that would never solve China’s most pressing health problem: the severe shortage of trained medical personnel. A 1931 League of Nations Health Organization survey had concluded that China would need 50,000 physicians in order to have just one doctor per 8,000 people.
Few as they were, the cadre of professionals produced by PUMC would play important roles in shaping China’s health system. In 1946 an observer wrote to Raymond Fosdick, commenting on the small number of PUMC graduates. “Both doctors and nurses are in positions of leadership and many of them are effective in leadership…we found plenty of evidence that this small group had had an influence quite out of proportion to its size.”
But many in China had expected more. A Chinese Ministry of Education assessment of PUMC in the mid-1930s urged not only that enrollment be increased but also that more classroom instruction be in Chinese. Other recommendations soon followed: increase the courses in public health, parasitology, and bacteriology; teach Chinese medical terminology; and publish papers in both Chinese and English so that they would reach a larger audience.
Henry Houghton, who had directed PUMC during its formative years in the 1920s, returned in 1934 to address these criticisms. But by the mid-1930s relations with some departments of the Chinese government had soured. Tensions between the New York office and PUMC had led to the firing of Roger Greene, and there were continuing difficulties in transforming PUMC into a more fully Chinese institution. By 1937 Houghton and his colleagues were making substantial moves toward bilingual instruction, reducing the numbers of Western faculty, and placing Chinese professors in positions of departmental leadership. Plans for a graduate medical school were also under discussion with the Ministry of Education, but the Japanese invasion in 1937 interrupted this work.
Surviving War and Revolution
At PUMC limited teaching continued for a time even though some prominent faculty and staff fled in 1937 to southwest China to assist with war-related training and rural health programs. The school closed completely only after the U.S. declaration of war on Japan in December 1941. The Japanese occupied the grounds of PUMC, imprisoning Houghton for the war’s duration. Heroically, the nurses moved their school in its entirety to Chengdu and reopened there in 1942.
PUMC resumed limited operations in 1947, but RF staff debated the Foundation’s role as nationalist and Communists factions fought for supremacy. Could they stay above the fray and continue their work? What was the Foundation’s role likely to be as a new political order took shape? Alan Gregg saw that Communism, which in the U.S. represented a challenge to capitalism, meant something else to the Chinese. Communism in China battled a feudal order. He concluded that this “puts American aid in combating Chinese Communism into some odd attitudes and curious commitments.”
In 1947, amid the uncertainty about PUMC’s future, the Foundation made a terminal grant of $10 million to the CMB. But in 1951 the People’s Republic of China nationalized PUMC and severed ties with the RF and CMB, Inc.
Between 1915 and 1951, the RF and CMB, Inc. spent well over $50 million on medical initiatives in China, nearly $45 million of it to establish PUMC. Other missionary hospitals benefited from smaller Foundation contributions. Fellowships helped doctors and nurses to travel abroad for advanced training. Medical texts were translated, and medical libraries were built. But the greatest RF legacy was PUMC and the enduring contributions its graduates have made to China’s health system. PUMC’s buildings, dedicated in 1921, still stand in the center of Beijing. A bust of JDR Sr. greets visitors to PUMC’s auditorium. The hospital still ranks as one of China’s most advanced. Today, the Chinese Academy of Medicine operates from the campus.
The Rockefeller Foundation and the birth of WHO
The launching of WHO in 1948 coincided with and helped stimulate the disbanding of the RF’s International Health Division (IHD) and the waning of the RF’s in international health. But, as we shall see, because the RF’s influence on international health’s institutions, ideologies, practices, and personnel was so pervasive from the 1910s through the 1940s, the WHO’s early years were imbued not only with the RF’s dominant technically-oriented disease-eradication model but also with its far more subordinate forays into social medicine, an approach grounded in political, economic, and social terms as much as the biomedical. – Source
During World War II, the LNHO was denuded of resources and staff (maintaining neutrality, while its rival, Paris-based Office International d’Hygie`ne Publique, in charge of sanitary conventions and surveillance, was accused of collaborating
with the Nazis).19 In 1943 the new US-sponsored and generously funded United Nations Relief and Rehabilitation Administration (UNRRA) largely absorbed and expanded upon
the LNHO’s functions through the massive provision of medical relief, sanitary services, and supplies in war-torn countries, with a staff of almost 1400 health professionals from some 40 countries and expenditures of up to $US80 million/year. UNRRA, too, had a deep RF imprint: it was devised and planned by IHD veteran Selskar Gunn, while IHD director Wilbur Sawyer became head of UNRRA health operations following his retirement from the RF in 1944.21 Not only were the LNHO and UNRRA the immediate precursors to WHO, they acted as a pipeline for WHO’s first generation of personnel. However, the hoped-for full transfer of funds to WHO upon UNRRA’s closing in 1947 consisted of a far more modest sum under five million dollars.
The Rockefeller Foundation pushed US into WHO
The RF was also invoked in the bitter US Congressional debate over joining WHO. Fearing that the country would repeat the error of not having joined the League of Nations, respected US Surgeon-General Thomas Parran (a presumed candidate for WHO director) gave impassioned testimony at the Senate on June 17, 1947: ‘Health has been termed by [RF President] Mr Raymond Fosdick as a ‘rallying point of unity’ in
international affairs. Cooperation . in the interest of health represents one of the most fruitful fields for international action. When one nation gains more of health it takes nothing away from any other nation. By learning how to work together in the interest of health, the lesson will be of value in other and more difficult fields.’
By this time the RF was busy mobilizing backstage in the context of unfolding Cold War rivalries. Rolf Struthers, Associate Director of the RF’s Medical Sciences Division, reported on his reconnaissance: ‘If U.S. insists on Parran . Russia will not join and it will not be a World Health Organization.’ This problem, together with the perception that Parran ‘does not enjoy wide support’ despite his distinction as a public health
leader, led IHD Director George Strode to suggest backing Chisholm ‘because he is thoroughly honest, understanding and deeply interested,’ although questions remained about his leadership effectiveness.
As late as March 12, 1948, the US Senate tabled a vote on WHO membership, leaving American public health leaders angry and embarrassed. The US finally joined WHO in July 1948 (almost three months after WHO’s April 7, 1948 ‘birthday’) following a compromise Joint Congressional resolution allowing the US to withdraw unilaterally from WHO on one year’s notice. Ironically, the USSR delegate formally proposed US
acceptance intoWHO, but it would be the USSR and Soviet bloc, not the US, that would later pull out of WHO (1949e1956).
With US membership settled, the RF began to judge the new organization’s first steps.
How the Rockefellers shaped the early WHO
Well into the 1950s the RF served in a retired emperor’s role, no longer the quotidian wielder of power but playing a crucial part behind the scenes in various ways. With the IHD’s impending demise, senior WHO administrators were keen that the RF’s Struthers spend a week in Geneva to get to know WHO technical staff, ‘learning both of their personalities and their fields of competence.’ Struthers found Chisholm ‘particularly anxious that the close association between the WHO and the RF’ continue, ‘both with the object of avoiding duplication of effort, and also that the RF was able to do some things which WHO could not do, and that our long experience, and objective and independent outlook were of value to the personnel of WHO.
A parade of RF officers was invited to serve on WHO expert committees, intensively so in the 1950s, and more sporadically in subsequent decades. After the IHD folded, RF staff wondered whether they should sit on WHO expert panels in areas that were no longer RF priorities, but DMPH director Warren assured them that such positions were useful for maintaining contacts, for example in malariology. Several RF nurses were asked to serve on the Expert Advisory Panel on Nursing, another colleague on the yellow fever panel in 1954, and so on. The RF was also involved in joint WHO/RF seminars in the early 1950s, supporting mostly travel costs to garner the interest of scientists in such areas as sanitary engineering.
A subset of RF men also became involved in WHO work in the areas of medical education, healthcare policy, and community health and development (the first two being major foci of the RF’s new DMPH). Launched with vigour under Chisholm,
this back door support for social medicine, even as WHO’s disease campaigns were proliferating, included: RF officer John Grant participating as ‘observer’ to the 1952 Expert Committee on Professional and Technical Education and various public health expert meetings through the 1950s; RF Vice President Alan Gregg serving on the Expert Panel on Medical Education in 1952; and panel membership of several leftwing social medicine experts who had been supported by the RF, such as Stampar and Sigerist. The reports produced by these panels made powerful recommendations about the need to incorporate comprehensive, community-based social welfare approaches rather than a narrow focus on clinical care.
In this regard, John Maier, a DMPH staff member, noted that WHO and the RF were facing similar dilemmas. At a WHO European study conference of Undergraduate Training in Hygiene, Preventive Medicine and Social Medicine, for example, Stampar although far more politically radical than his patrons outlined the difficulties caused by a ‘separation and antagonism between preventive and curative medicine’ and suggested calling medical schools ‘schools of health.
The RF’s effort to undo its longstanding compartmentalization of medicine and public health was partially linked to WHO, involving for example, RF support for several medical schools in Colombia, which in the 1960s informed WHO’s call for the teaching of community-based, preventive, social and occupational medicine as part of internationally accepted standards.
In the early 1950s, Grant was at the fulcrum of RF-WHO collaborative social medicine efforts. His commissioned paper on the ‘International Planning of Organization for
Medical Care,’ was presented before WHO’s Department of Advisory Services in 1951, informing the recommendations of related expert panels.77 This work emphasized the importance of regionalized health systems and village health committees. Later that year he was nominated by WHO to be a member (funded by the RF) of a three-person UN survey mission on community organization and development in India, Ceylon (now Sri Lanka), Thailand, and the Philippines.
The survey, building on Grant’s prior scouting of inter-agency cooperation possibilities among WHO, UNICEF, and the US government to ‘rebuild’ Southeast Asia,78 highlighted the economic and social aspects of community programs, again stressing self-help efforts, in part as a means of fending off communism.
9 WHO’s European office was also keen to have Grant’s participation, inviting him on a study tour of Sweden, Scotland, and Belgium,80 and receiving almost $US50,000 from
the RF over three years to study personnel needs under Europe’s new health and social welfare laws. Grant observed that some believed that they were so far advanced, there was little room for improvement, with Norway and Sweden serving as paradoxical ‘exceptions to this attitude.’
By the mid-1950s, RF leaders believed that the RF need no longer be represented at every WHO meeting and ‘should maintain good relations and reasonably close contact.
Soon enough, WHO invitations for RF participation were turned down.
With its resources now focused elsewhere, the RF sought to rally other philanthropic players. It had already tested these waters in 1949, suggesting that WHO approach the Ford Foundation for a subsidy towards a new building, and in early 1951, the RF and the Kellogg Foundation each provided PASB with $US150,000 interest free loans to purchase a building to serve as headquarters.86 Kellogg also joined the RF in providing fellowships.
The role of the RF’s flagship fellowship program was an important ongoing issue. At first, the IHD sought to retain public health fellowships ‘in significant fields which are not major interests of WHO’ because of WHO’s tendency to let member countries select fields and individuals for fellowships, which might ‘preclude senior men who may be
developing newer areas. The RF also questioned WHO’s preference for fellowships to be held at non-US schools, a policy WHO justified by the large number of foreign students attending these institutions. Another problem was due to WHO’s poaching of fellows who had been trained specifically for RF projects. The RF called for mutual ‘consideration and unusual courtesies,’ meaning that WHO should ‘refrain from offering attractive employment’ to men destined for RF work.
Chisholm was so alarmed by these personnel raiding accusations that he sought RF permission to use the RF fellowship directory to recruit candidates for field projects.
The RF was careful not to bankroll WHO projects without participating in their design. DMPH director Warren was particularly troubled by a request that it work with WHO to
support Manila’s Institute of Hygiene, declaring, ‘the only categorical statement I can make is that we will not operate through WHO or any other intermediary.’ The DMPH ultimately granted $US20,000 but only to support visiting Johns Hopkins faculty. By 1952 it was mutually decided that there would be ‘no further joint projects, but that we will maintain a relatively close liaison’ in training courses in insect control and biological testing of insecticides.94 On the other hand, the RF sought to take advantage of WHO demonstration projects to organize particular studies.
Despite these changes, the RF remained on the pulse of WHO politics. Numerous Americans involved in WHO confided to RF staff about developments under Chisholm.
Some were concerned with decentralized regionalization; others believed that Henry Sigerist, self-exiled from Johns Hopkins back to Switzerland, was exerting ‘undue influence’ public health on Chisholm in regards to both national health insurance
and medical education reform.96 Grant, meanwhile, kept a close eye on social medicine developments and praised WHO’s increasing emphasis on program evaluation. But his critique of technical assistance in Thailand was met by defensive WHO staff intent on gaining RF understanding and approval.
In 1952, the big storm was around Norwegian Executive Board chair Karl Evang’s speech and motion on WHO’s recognition of and involvement in population studies and
control of reproduction. A ‘highly emotional controversy’ ensued over the following days, with France, Belgium, Ireland, and Italy threatening to resign from WHO. Following a ‘tense debate,’ these countries, facing ‘religious political pressure,’
defeated attempts at any technical discussions: Evang’s motion was not brought to a vote but advisory birth control work in India was allowed to continue.
This incident, which nearly broke WHO apart, also delineated an area for RF work that would not overlap with WHO efforts. Just a month later, John D Rockefeller III convened an invitation-only ‘Conference on Population Problems’ with top experts.He founded the Population Council shortly thereafter, separately from the RF because its own board was divided, thus partially (though not intentionally) shielding WHO from this problematic arena.
Another difficulty faced by the young WHO was financial.
In both 1953 and 1954, the US paid only $US8 million of $US12 million pledged, even while the UN had asked WHO to increase its technical assistance to member countries. With a $US30 million shortfall, WHO was forced to freeze spending.
One RF officer berated, ‘The WHO is just learning the wisdom of setting aside all funds for each project out of current budget.’105 RF staff also learned that WHO was fearful of the ‘empire-building aspects’ of UNICEF, which was more solidly (largely US) funded and ‘will tend to use its stronger autonomous position’ to build its own technical staff rather than rely on WHO as per the original agreement.
Concerns about the urgency of US support for WHO were so great that advocates approached the RF for help from all angles. Esteemed US public health man Frank Boudreau (who rose to deputy director of the LNHO and then executive director of the Milbank Memorial Fund), chair of the National Citizens Committee for World Health, appealed to Nelson Rockefeller107 to attend the National Conference on World Health in 1953. The Committee, set up in 1951 to generate public interest and support for international health and save the United Nations from the fate of the League of Nations,
already had Chisholm, Eleanor Roosevelt, the US SurgeonGeneral, and RF President Dean Rusk lined up as speakers at its conference, but the presence of a Rockefeller family member was deemed essential
The RF’s stamp on WHO was reinforced with the May 1953 election of Dr. Marcolino Candau as its director-general.
Candau had been an RF fellow and had worked with Soper in IHD’s Anopheles gambiae campaign in Brazil, then briefly served as his deputy at PASB. Initially there were close interactions. Grant learned early that Chisholm would be resigning in June 1953, after a single term. Because of Soper’s continued relations with former colleagues, the RF was privy to the internal battles and ‘considerable hard feelings’ over Chisholm’s successor. With British support for a Pakistani candidate and Vatican support for an Italian, ‘through Chisholm’s intervention, and after very close voting, Candau of Brazil was nominated, and presumably will be elected.’110 Soper ‘has confidence’ that Candau would ‘bring strong leadership to WHO Secretariat.
In October 1954, new RF President Dean Rusk invited Candau for lunch and a
‘relaxed discussion’ about WHO programs and ‘what a private organization might do in the world today in the field of medical education and medical care.’ Candau suggested RF support for education, research, and training in strong regional institutions such as Mexico’s Institute of Cardiology, the Sao Paulo and Santiago schools of public health, and the new Central American Institute of Nutrition. Rusk saved the ‘Mars bars’ question for after dessert: Candau’s position on birth control. After pretending he had to leave, Candau explained that he had been instructed to keep mum on this issue, though he was well aware of the ‘population-food problem’ and that other UN agencies were accusing WHO of ‘creating more problems than it was solving.’ As such, Candau argued, birth
control work was well-suited to private organizations.
Once the RF became satisfied with Candau’s agenda for WHO, more routine matters resumed. Tensions over fellowships resurfaced under Candau because the RF was getting growing numbers of WHO staff applications for fellowships that had not been approved institutionally. Candau lobbied several RF men, hoping for ‘sympathetic consideration’ so that a few outstanding fellows could become key personnel for permanent WHO positions, both at headquarters and regional offices. He also wrote DMPH director Warren, promising to screen all candidates, and hoping for continued
support: ‘It is fully realized that you cannot envisage continuing the granting of fellowships for an indefinite period.
We are, however, most grateful for your agreeing to assist WHO in the development of its staff during these early critical years.’120 RF staff suspected Candau wanted much of WHO staff trained at RF expense and ‘is now trying to hedge a bit on his agreement in the hope that he can wangle more fellowships than you had in mind..Hence, the training program would seem to be a more or less continuous process.
Warren concluded the discussion by promising: ‘As you know, we are anxious to do all we can to help you and your colleagues . develop a sound corps of well-trained people for permanent and long term work. [but] Because of limited funds, and need to train personnel closer to home, [we] will not support operating field personnel. For a few years, new RF-WHO fellowships again rose, going from 2 in 1953 to 8 in 1959, but by 1963 there was only 1, in 1964 2, and only 1 new RF fellow from WHO in 1968.123 By this time the WHA had approved major funding for fellowships,124 and the RF was no
longer needed.
In 1955 another conflict brewed around WHO’s job offer to the director of an RF-funded community health centre in France. John Maier, now an assistant RF division director,
wanted to draft a harsh letter to Candau about the matter but was told this was ‘inadvisable,’ and he would ‘simply have to grin and bear it.’126 Further confidential, high level discussions about the case called for informal approaches: ‘It was decided
that the RF was not justified in taking such a stand.on the basis that we should not try to play God.’
Around this juncture, the RF-WHO relationship began to grow more distant. The New York meeting with Rusk led to unofficial RF approval of Candau’s indefinite posting as
director-general, which lasted until 1973. Candau oversaw the establishment of WHO’s global malaria and smallpox eradication campaigns, a growing WHO bureaucracy, and a massive effort to provide public health training fellowships to over 50,000 health personnel from across the world.
Ironically, or perhaps due to this connection, the late 1950s and 1960s was the period of least interaction between the RF and WHO. To be sure, Soper was a central shaper of its malaria campaign, and Paul Russell and other RF men were involved. But the growth in membership of WHO following the liberation struggles of dozens of new nations in
Africa and Asia (and later, the Caribbean), accompanied by increasing bureaucratization, and the malaria effort e significantly financed by the US government (and a few others) through ‘voluntary’ contributions rather than regular member country dues, moved the RF further away from WHO’s centre stage. The RF’s period as prime advisor was over and WHO went from being swayed by the priorities and agenda of the foundation to becoming subject to powerful, far larger donors, most notably the United States, in the context of Cold War exigencies.
Certain collaborations did continue. In 1958 the RF granted $US25,000 for a WHO manual of operations.129 Joint efforts, such as $US250,000 in RF support for research to combat protein malnutrition carried out in 12 countries, involved WHO in an advisory capacity, among other agencies. In 1960 the RF’s new Division of Medical and Natural Sciences joined WHO to support a rural public health centre in Kenya and a School of Nursing in Congo Republic, as well as various efforts in medical education. As in the past, numerous RF-trained and supported experts from around the world rose to prominent positions at WHO.
But the RF began to turn down WHO requests as often as it accepted them, and focused on narrowly targeted efforts such as funding a WHO bibliography on hookworm.133 For its part, WHO was also reluctant to commit to co-sponsoring RF projects. When USAID administrator Leona Baumgartner suggested in 1963 that USAID, the RF, and WHO carry out a joint study on training of ancillary health personnel and staffing needs, Candau offered support of a WHO statistician but insisted ‘WHO cannot be considered as a Sponsoring Agency.’
Meanwhile, the RF had also changed tolerance of social medicine on the margins of its main efforts dwindled with Alan Gregg’s and John Grant’s respective retirement and death and amidst the continued red-baiting of the McCarthy era. For example, since his posting by the RF to Puerto Rico in 1954 to set up a coordinated medical and public health system of research and practice,36 Grant had been keen to make WHO aware ‘that their present categorical activities must be replaced by polyvalent permanent local organizations.
After four years, a possibility finally materialized only circuitously when the National Citizens Committee for the World Health Organization obtained grants from the RF, as well as the Milbank, Kellogg, and Avalon foundations and various industrial concerns, to fund key public health delegates to the 1958 WHA (held in Minneapolis) to travel to Puerto Rico to attend a series of professional sessions arranged by Grant and see the island’s ‘progressive public health and medical services.’136 But this was an anomalous episode: after 1954, the RF’s European office (a vital link to WHO) shrank by 90% and
public health RF programming moved even further away from public and international health (though support for bench research on arboviruses and other tropical diseases, and some community medicine efforts, continued apace).
From backstage to backdrop It is not surprising that the RF left such a deep impression on WHO, for the IHD was the most influential international health actor of the era. Before WWII, European powers were focused on their colonial networks, with inter-imperial commercial rivalries impeding strong international agencies, while the US government was testing its own international health leadership in the Americas. Thus by default and through its own protagonism, the RF was the de facto international health leader. Even after the IHD closed down shortly after WHO was founded, this was no disappearing act. The RF’s disease control ideology and approach to international health were infused into the agenda and practices of WHO. This took place both directly, through the discreet advice it purveyed and the generations of RF personnel and numerous RF fellows and grantees WHO employed and consulted, and indirectly, through the RF having shaped the international health scene via scores of in-country cooperative efforts over almost forty years and through its hand in designing and supporting major multilateral health institutions over several decades.
What is remarkable is that not only was the RF’s predominant technobiological paradigm adopted by WHO, but so was its modest entre´e into social medicine, advanced by a small contingent of left-leaning longtime IHD officers. This was
particularly marked during WHO’s early years, when Chisholm, himself not an RF man, opened the organization to this alternative perspective even as the RF’s main approach bore down on his administration. In those years, the RF was subtly ever present conveying both of its legacies, albeit at different scales.
How and why the RF subsequently became less visible at WHO also illuminates the constraints of shifting power blocs at WHO. The bulk of Candau’s period would mark a distancing between WHO and the RF, even as the RF’s disease control model had become fully entrenched at WHO, most visibly through the launching of the global malaria eradication campaign. On one level, this paradoxdCandau’s rise coinciding with the RF’s demise at WHO indicated that because its approach was firmly in place at WHO, the RF’s presence was superfluous.
On another level, this estrangement meant that some openings to social medicine enabled by the RFeWHO relationship now faded. While RF-sponsored advocates of social medicine remained on certain expert committees, the hard line of McCarthyism wiped out many American health leftists in particular. A notable target was health systems and policy expert Milton Roemer, who left the repressive context of the United States to work at WHO in 1950, only to lose his WHO appointment in 1953 after the US government revoked his passport due to his refusal to sign a loyalty oath.137 In the late
1950s and 1960s, some social medicine advocates involved in WHO came from other quarters, including Latin America and Africa. Sidney and Emily Kark, for example, who had innovated a successful community health centre model in South Africa (in part thanks to RF officer John Grant’s backing), participated in various WHO activities. But under Candau and with heightened Cold War rivalries at WHO sparked by the return to active membership of the Soviet bloc in the mid1950s, this health internationalist tenor was marginalized at WHO, only to resurface, as we shall see in Part II, starting in the late 1960s and early 1970s.
The RF became but a backdrop not only at WHO but also on the international health scene writ large. Indeed, the subtitle of a 1959 US Senate report about the US and WHO, ‘Teamwork for Mankind’s Well-Being,’130 echoed, perhaps inadvertently, the RF’s 1913 motto: ‘For the Well-Being of Mankind throughout the World.’ This 150-page document cited the RF’s link to WHO on just two pages and only in regards to interagency research collaboration, with no mention of the RF’s pivotal prior role in setting the international health agenda.
The importance of the RF’s advocacy, legitimacy, and seed funding for projects diminished considerably after the US’s financial support of WHO efforts soared starting in 1956-7, in the wake of the influenza pandemic, the Soviet bloc rejoining
WHO, and US recognition of the potential of the malaria eradication campaign to combat communism. As such, the RF’s organizational power was waning even as its ideological approach to international health had become solidly institutionalized within WHO.
In sum, the Rockefeller Foundation had enormous bearing on WHO, just as it did on the overall international health arena: WHO’s very configuration was unthinkable without the RF. Yet as WHO found firm ground in the 1950s and the RF abandoned its primordial international health role, there was a tacit understanding that the RF would not interfere in day-to-day operations, even as WHO leaders and champions remained conscious of the RF’s underlying influence. After the US government brashly moved onto WHO’s turf at the height of the Cold War, particularly through its role in the global malaria eradication campaign, there was a further distancing between the RF and WHO.
Backstage: the relationship between the Rockefeller
As will be discussed in Part II, it was only in the 1970s that the relationship resumed, just when WHO began to question the RF’s disease campaign model, and, backed by the bulk of its member countries, it pursued a more community-grounded approach to primary health care amidst calls for a new antihegemonic economic order. By this time, the RF’s support for such social justice-oriented efforts was much narrowed in the context of the dominant ideological shift towards neoliberalism, and it played what many perceived as an antagonistic role in seeking to resurrect its disease control paradigm.
Foundation and the World Health Organization,
Part I: 1940se1960s by A.-E. Birn – 2013 The Royal Society for Public Health
To be continued?
Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production.
Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them

We think frequent mask use, even short term use can be bad for you, but if you have no way around them, at least send a message of consciousness.
Get it here!
