New plan aims to accelerate research translation, advance equity
Today, on National Nanotechnology Day, the White House Office of Science and Technology Policy (OSTP) and the National Nanotechnology Coordination Office (NNCO) unveiled the 2021 National Nanotechnology Initiative (NNI) Strategic Plan. This strategy details a new framework to ensure that the United States continues to lead the world not only in nanoscience discoveries, but in translating and manufacturing its products to benefit all of America. In addition to identifying priorities for the NNI to best support the research community in the United States, the plan prioritizes efforts to expand sustainable infrastructure and advance equity in the nanotechnology workforce.
“The role of nanotechnology in our response to the pandemic—from vaccine delivery to protective clothing to testing kits—emphasizes the potential for small science to have big impacts,” said National Nanotechnology Coordination Office Director Dr. Lisa E. Friedersdorf. “This strategic plan charts an exciting path forward for the National Nanotechnology Initiative to ensure continued progress in nanotechnology research and development, and to attract students from across all of America.”
Nanotechnology research and development requires access to specialized tools and facilities. This plan emphasizes the need to expand and refresh the research infrastructure, and provide access that supports researchers and small business across all of America. This research infrastructure also plays a critical role in training the future workforce for high-paying jobs.
Since the launch of the NNI in 2000, nanoscience has transformed from an emerging area of research to a technology that is fueling real-world applications in areas as diverse as consumer electronics, water purification, infrastructure, medicine, energy, space exploration, and agriculture. Nanotechnology underpins and enables other critical technologies, including quantum computing and artificial intelligence, and will also help address the most significant challenges facing the world, including pandemic preparedness, climate change, and food insecurity. This strategic plan lays out a path to ensure continued U.S. leadership in this important area.
More on the National Nanotechnology Initiative (NNI): The NNI was announced in 2000 and codified on Dec. 3, 2003, through the 21st Century Nanotechnology Research and Development Act (15 USC §7501), to enhance interagency coordination of nanotechnology research and development; support a shared infrastructure; enable leveraging of resources while avoiding duplication; and establish shared goals, priorities, and strategies that complement agency-specific missions and activities.
More information on the NNI, including upcoming events and opportunities to engage, is available on Nano.gov. Inquiries and comments also can be sent to info@nnco.nano.gov.
###
This above is probably why some people attribute this to Biden’s admin. They\ve never come out with anything new and original, not even that oxymoronic “Build Back Better” slogan. This dates back to the Clinton admin, and originates in military research:
“Mihail C. Roco proposed the initiative in a 1999 presentation to the White House under the Clinton administration. The NNI was officially launched in 2000 and received funding for the first time in FY2001.
President Bill Clinton advocated nanotechnology development. In a 21 January 2000 speech at the California Institute of Technology, Clinton stated that “Some of our research goals may take twenty or more years to achieve, but that is precisely why there is an important role for the federal government.”
President George W. Bush further increased funding for nanotechnology. On 3 December 2003 Bush signed into law the 21st Century Nanotechnology Research and Development Act (Pub. L.108–153 (text)(PDF)), which authorizes expenditures for five of the participating agencies totaling $3.63 billion over four years. This law is an authorization, not an appropriation, and subsequent appropriations for these five agencies have not met the goals set out in the 2003 Act. However, there are many agencies involved in the Initiative that are not covered by the Act, and requested budgets under the Initiative for all participating agencies in Fiscal Years 2006 – 2015 totaled over $1 billion each.
In February 2014, the National Nanotechnology Initiative released a Strategic Plan outlining updated goals and “program component areas”, as required under the terms of the Act. This document supersedes the NNI Strategic Plans released in 2004 and 2007.
The NNI’s budget supplement proposed by the Obama administration for Fiscal Year 2015 provides $1.5 billion in requested funding. The cumulative NNI investment since fiscal year 2001, including the 2015 request, totals almost $21 billion. Cumulative investments in nanotechnology-related environmental, health, and safety research since 2005 now total nearly $900 million. The Federal agencies with the largest investments are the National Institutes of Health, National Science Foundation, Department of Energy, Department of Defense, and the National Institute of Standards and Technology.
The NNI cumulative investment by 2021 inclusive reached $36 billion, and nanotechnology has become pervasive in material, energy and biosystem related applications.”
Where we learn that the invention of the Lipid Nano-Containers used in Covid mRNA vaccines was publicly-funded research, Pfizer and Moderna just parasiting government’s achievements and selling it back to the people, “the owners of the Government”, at astronomical prices.
Here’s something to further support for our findings that legal drug dealers and arms dealers are not really separate cartels, but rather form a Military BioTech Complex, that also includes the Silicone Valley freaks:
This timeline features Premodern example of nanotechnology, as well as Modern Era discoveries and milestones in the field of nanotechnology.
Premodern Examples of Nanotechnologies
Early examples of nanostructured materials were based on craftsmen’s empirical understanding and manipulation of materials. Use of high heat was one common step in their processes to produce these materials with novel properties.
The Lycurgus Cup at the British Museum, lit from the outside (left) and from the inside (right)
4th Century: The Lycurgus Cup (Rome) is an example of dichroic glass; colloidal gold and silver in the glass allow it to look opaque green when lit from outside but translucent red when light shines through the inside. (Images at left.)
The South rose window of Notre Dame Cathedral, ca 1250
6th-15th Centuries: Vibrant stained glass windows in European cathedrals owed their rich colors to nanoparticles of gold chloride and other metal oxides and chlorides; gold nanoparticles also acted as photocatalytic air purifiers. (Image at left.)
13th-18th Centuries:“Damascus” saber blades contained carbon nanotubes and cementite nanowires—an ultrahigh-carbon steel formulation that gave them strength, resilience, the ability to hold a keen edge, and a visible moiré pattern in the steel that give the blades their name. (Images below.)
(Left) A Damascus saber (photo by Tina Fineberg for The New York Times). (Right) High-resolution transmission electron microscopy image of carbon nanotubes in a genuine Damascus sabre after dissolution in hydrochloric acid, showing remnants of cementite nanowires encapsulated by carbon nanotubes (scale bar, 5 nm) (M. Reibold, P. Paufler, A. A. Levin, W. Kochmann, N. Pätzke & D. C. Meyer, Nature 444, 286, 2006).
Examples of Discoveries and Developments Enabling Nanotechnology in the Modern Era
These are based on increasingly sophisticated scientific understanding and instrumentation, as well as experimentation.
“Ruby” gold colloid (Gold Bulletin 2007 40,4, p. 267)
1857: Michael Faraday discovered colloidal “ruby” gold, demonstrating that nanostructured gold under certain lighting conditions produces different-colored solutions.
1936: Erwin Müller, working at Siemens Research Laboratory, invented the field emission microscope, allowing near-atomic-resolution images of materials.
1947: John Bardeen, William Shockley, and Walter Brattain at Bell Labs discovered the semiconductor transistor and greatly expanded scientific knowledge of semiconductor interfaces, laying the foundation for electronic devices and the Information Age.
1947 transistor, Bell Labs
1950: Victor La Mer and Robert Dinegar developed the theory and a process for growing monodisperse colloidal materials. Controlled ability to fabricate colloids enables myriad industrial uses such as specialized papers, paints, and thin films, even dialysis treatments.
1951: Erwin Müller pioneered the field ion microscope, a means to image the arrangement of atoms at the surface of a sharp metal tip; he first imaged tungsten atoms.
1956: Arthur von Hippel at MIT introduced many concepts of—and coined the term—“molecular engineering” as applied to dielectrics, ferroelectrics, and piezoelectrics
Jack Kilby, about 1960.
1958: Jack Kilby of Texas Instruments originated the concept of, designed, and built the first integrated circuit, for which he received the Nobel Prize in 2000. (Image at left.)
Richard Feynman (Caltech archives)
1959: Richard Feynman of the California Institute of Technology gave what is considered to be the first lecture on technology and engineering at the atomic scale, “There’s Plenty of Room at the Bottom” at an American Physical Society meeting at Caltech. (Image at right.)
1965: Intel co-founder Gordon Moore described in Electronics magazine several trends he foresaw in the field of electronics. One trend now known as “Moore’s Law,” described the density of transistors on an integrated chip (IC) doubling every 12 months (later amended to every 2 years). Moore also saw chip sizes and costs shrinking with their growing functionality—with a transformational effect on the ways people live and work. That the basic trend Moore envisioned has continued for 50 years is to a large extent due to the semiconductor industry’s increasing reliance on nanotechnology as ICs and transistors have approached atomic dimensions.1974: Tokyo Science University Professor Norio Taniguchi coined the term nanotechnology to describe precision machining of materials to within atomic-scale dimensional tolerances. (See graph at left.)
1981: Gerd Binnig and Heinrich Rohrer at IBM’s Zurich lab invented the scanning tunneling microscope, allowing scientists to “see” (create direct spatial images of) individual atoms for the first time. Binnig and Rohrer won the Nobel Prize for this discovery in 1986.
1981: Russia’s Alexei Ekimov discovered nanocrystalline, semiconducting quantum dots in a glass matrix and conducted pioneering studies of their electronic and optical properties.
1985: Rice University researchers Harold Kroto, Sean O’Brien, Robert Curl, and Richard Smalley discovered the Buckminsterfullerene (C60), more commonly known as the buckyball, which is a molecule resembling a soccer ball in shape and composed entirely of carbon, as are graphite and diamond. The team was awarded the 1996 Nobel Prize in Chemistry for their roles in this discovery and that of the fullerene class of molecules more generally. (Artist’s rendering at right.)
1985: Bell Labs’s Louis Brus discovered colloidal semiconductor nanocrystals (quantum dots), for which he shared the 2008 Kavli Prize in Nanotechnology.
1986: Gerd Binnig, Calvin Quate, and Christoph Gerber invented the atomic force microscope, which has the capability to view, measure, and manipulate materials down to fractions of a nanometer in size, including measurement of various forces intrinsic to nanomaterials.
1989: Don Eigler and Erhard Schweizer at IBM’s Almaden Research Center manipulated 35 individual xenon atoms to spell out the IBM logo. This demonstration of the ability to precisely manipulate atoms ushered in the applied use of nanotechnology. (Image at left.)
1990s:Early nanotechnology companies began to operate, e.g., Nanophase Technologies in 1989, Helix Energy Solutions Group in 1990, Zyvex in 1997, Nano-Tex in 1998….
1991: Sumio Iijima of NEC is credited with discovering the carbon nanotube (CNT), although there were early observations of tubular carbon structures by others as well. Iijima shared the Kavli Prize in Nanoscience in 2008 for this advance and other advances in the field. CNTs, like buckyballs, are entirely composed of carbon, but in a tubular shape. They exhibit extraordinary properties in terms of strength, electrical and thermal conductivity, among others. (Image below.)
Carbon nanotubes (courtesy, National Science Foundation). The properties of CNTs are being explored for applications in electronics, photonics, multifunctional fabrics, biology (e.g., as a scaffold to grow bone cells), and communications. See a 2009 Discovery Magazine article for other examples
SEM micrograph of purified nanotube “paper” in which the nanotubes are the fibers (scale bar, 0.001 mm) (courtesy, NASA).
An array of aligned carbon nanotubes, which can act like a radio antenna for detecting light at visible wave- lengths (scale bar 0.001 mm) (courtesy, K. Kempa, Boston College).
1992: C.T. Kresge and colleagues at Mobil Oil discovered the nanostructured catalytic materials MCM-41 and MCM-48, now used heavily in refining crude oil as well as for drug delivery, water treatment, and other varied applications.
MCM-41 is a “mesoporous molecular sieve” silica nanomaterial with a hexagonal or “honeycomb” arrangement of its straight cylindrical pores, as shown in this TEM image (courtesy of Thomas Pauly, Michigan State University).
This TEM image of MCM-41 looks at the straight cylindrical pores as they lie perpendicular to the viewing axis (courtesy of Thomas Pauly, Michigan State University).
1993: Moungi Bawendi of MIT invented a method for controlled synthesis of nanocrystals (quantum dots), paving the way for applications ranging from computing to biology to high-efficiency photovoltaics and lighting. Within the next several years, work by other researchers such as Louis Brus and Chris Murray also contributed methods for synthesizing quantum dots.
1998: The Interagency Working Group on Nanotechnology (IWGN) was formed under the National Science and Technology Council to investigate the state of the art in nanoscale science and technology and to forecast possible future developments. The IWGN’s study and report, Nanotechnology Research Directions: Vision for the Next Decade (1999) defined the vision for and led directly to formation of the U.S. National Nanotechnology Initiative in 2000.
The progression of steps of using a scanning tunneling microscope tip to “assemble” an iron carbonyl molecule, beginning with Fe (iron) and CO (carbon monoxide) molecules (A), joining them to produce FeCO (B), then adding a second CO molecule (C), to achieve the FECO2 molecule (D). (H.J. Lee, W. Ho, Science 286, 1719 [1999].)
1999: Cornell University researchers Wilson Ho and Hyojune Lee probed secrets of chemical bonding by assembling a molecule [iron carbonyl Fe(CO)2] from constituent components [iron (Fe) and carbon monoxide (CO)] with a scanning tunneling microscope. (Image at left.)
1999: Chad Mirkin at Northwestern University invented dip-pen nanolithography® (DPN®), leading to manufacturable, reproducible “writing” of electronic circuits as well as patterning of biomaterials for cell biology research, nanoencryption, and other applications. (Image below right.)
1999–early 2000’s:Consumer products making use of nanotechnology began appearing in the marketplace, including lightweight nanotechnology-enabled automobile bumpers that resist denting and scratching, golf balls that fly straighter, tennis rackets that are stiffer (therefore, the ball rebounds faster), baseball bats with better flex and “kick,” nano-silver antibacterial socks, clear sunscreens, wrinkle- and stain-resistant clothing, deep-penetrating therapeutic cosmetics, scratch-resistant glass coatings, faster-recharging batteries for cordless electric tools, and improved displays for televisions, cell phones, and digital cameras.
2000: President Clinton launched the National Nanotechnology Initiative (NNI) to coordinate Federal R&D efforts and promote U.S. competitiveness in nanotechnology. Congress funded the NNI for the first time in FY2001. The NSET Subcommittee of the NSTC was designated as the interagency group responsible for coordinating the NNI.
2003: Congress enacted the 21st Century Nanotechnology Research and Development Act (P.L. 108-153). The act provided a statutory foundation for the NNI, established programs, assigned agency responsibilities, authorized funding levels, and promoted research to address key issues.
Computer simulation of growth of gold nanoshell with silica core and over-layer of gold (courtesy N. Halas, Genome News Network, 2003)
2003: Naomi Halas, Jennifer West, Rebekah Drezek, and Renata Pasqualin at Rice University developed gold nanoshells, which when “tuned” in size to absorb near-infrared light, serve as a platform for the integrated discovery, diagnosis, and treatment of breast cancer without invasive biopsies, surgery, or systemically destructive radiation or chemotherapy.2004: The European Commission adopted the Communication “Towards a European Strategy for Nanotechnology,” COM(2004) 338, which proposed institutionalizing European nanoscience and nanotechnology R&D efforts within an integrated and responsible strategy, and which spurred European action plans and ongoing funding for nanotechnology R&D. (Image at left.)
2004: Britain’s Royal Society and the Royal Academy of Engineering published Nanoscience and Nanotechnologies: Opportunities and Uncertainties advocating the need to address potential health, environmental, social, ethical, and regulatory issues associated with nanotechnology.
2005: Erik Winfree and Paul Rothemund from the California Institute of Technology developed theories for DNA-based computation and “algorithmic self-assembly” in which computations are embedded in the process of nanocrystal growth.
2006: James Tour and colleagues at Rice University built a nanoscale car made of oligo(phenylene ethynylene) with alkynyl axles and four spherical C60 fullerene (buckyball) wheels. In response to increases in temperature, the nanocar moved about on a gold surface as a result of the buckyball wheels turning, as in a conventional car. At temperatures above 300°C it moved around too fast for the chemists to keep track of it! (Image at left.)
2007: Angela Belcher and colleagues at MIT built a lithium-ion battery with a common type of virus that is nonharmful to humans, using a low-cost and environmentally benign process. The batteries have the same energy capacity and power performance as state-of-the-art rechargeable batteries being considered to power plug-in hybrid cars, and they could also be used to power personal electronic devices. (Image at right.)
(L to R) MIT professors Yet-Ming Chiang, Angela Belcher, and Paula Hammond display a virus-loaded film that can serve as the anode of a battery. (Photo: Donna Coveney, MIT News.)
2009–2010: Nadrian Seeman and colleagues at New York University created several DNA-like robotic nanoscale assembly devices. One is a process for creating 3D DNA structures using synthetic sequences of DNA crystals that can be programmed to self-assemble using “sticky ends” and placement in a set order and orientation. Nanoelectronics could benefit: the flexibility and density that 3D nanoscale components allow could enable assembly of parts that are smaller, more complex, and more closely spaced. Another Seeman creation (with colleagues at China’s Nanjing University) is a “DNA assembly line.” For this work, Seeman shared the Kavli Prize in Nanoscience in 2010.
2010: IBM used a silicon tip measuring only a few nanometers at its apex (similar to the tips used in atomic force microscopes) to chisel away material from a substrate to create a complete nanoscale 3D relief map of the world one-one-thousandth the size of a grain of salt—in 2 minutes and 23 seconds. This activity demonstrated a powerful patterning methodology for generating nanoscale patterns and structures as small as 15 nanometers at greatly reduced cost and complexity, opening up new prospects for fields such as electronics, optoelectronics, and medicine. (Image below.)
A rendered image of a nanoscale silicon tip chiseling out the smallest relief map of the world from a substrate of organic molecular glass. Shown middle foreground is the Mediterranean Sea and Europe. (Image courtesy of Advanced Materials.)
2012: The NNI launched two more Nanotechnology Signature Initiatives (NSIs)–Nanosensors and the Nanotechnology Knowledge Infrastructure (NKI)–bringing the total to five NSIs.
2013: -The NNI starts the next round of Strategic Planning, starting with the Stakeholder Workshop. -Stanford researchers develop the first carbon nanotube computer.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Sometimes my memes are 3D. And you can own them. Or send them to someone. You can even eat some of them. CLICK HERE
We’ve all heard of existing cancer cures, whether you believe in them or not, you can’t rationally hope they will be made available to plebs for as long a Pharmafia exists.
Goldman Sachs asks in biotech research report: ‘Is curing patients a sustainable business model?’
Goldman Sachs analysts attempted to address a touchy subject for biotech companies, especially those involved in the pioneering “gene therapy” treatment: cures could be bad for business in the long run.
“Is curing patients a sustainable business model?” analysts ask in an April 10 report entitled “The Genome Revolution.”
“The potential to deliver ‘one shot cures’ is one of the most attractive aspects of gene therapy, genetically-engineered cell therapy and gene editing. However, such treatments offer a very different outlook with regard to recurring revenue versus chronic therapies,” analyst Salveen Richter wrote in the note to clients Tuesday. “While this proposition carries tremendous value for patients and society, it could represent a challenge for genome medicine developers looking for sustained cash flow.”
Richter cited Gilead Sciences’ treatments for hepatitis C, which achieved cure rates of more than 90 percent. The company’s U.S. sales for these hepatitis C treatments peaked at $12.5 billion in 2015, but have been falling ever since. Goldman estimates the U.S. sales for these treatments will be less than $4 billion this year, according to a table in the report.
“Gilead is a case in point, where the success of its hepatitis C franchise has gradually exhausted the available pool of treatable patients,” the analyst wrote. “In the case of infectious diseases such as hepatitis C, curing existing patients also decreases the number of carriers able to transmit the virus to new patients, thus the incident pool also declines … Where an incident pool remains stable (eg, in cancer) the potential for a cure poses less risk to the sustainability of a franchise.”
The analyst didn’t immediately respond to a request for comment.
The report suggested three potential solutions for biotech firms:
“Solution 1: Address large markets: Hemophilia is a $9-10bn WW market (hemophilia A, B), growing at ~6-7% annually.”
“Solution 2: Address disorders with high incidence: Spinal muscular atrophy (SMA) affects the cells (neurons) in the spinal cord, impacting the ability to walk, eat, or breathe.”
“Solution 3: Constant innovation and portfolio expansion: There are hundreds of inherited retinal diseases (genetics forms of blindness) … Pace of innovation will also play a role as future programs can offset the declining revenue trajectory of prior assets.”
So you don’t see anyone pushing for any cures.
CONSUMER AFFAIRS
Biden’s moonshot examined: Researchers say cancer cure is a long ways off
The White House is pressing ahead, saying a combination of research on cures and prevention efforts will end the scourge.
Congress has appropriated $1.8 billion for the “cancer moonshot” President Joe Biden began in 2016, and the positive reaction to Biden’s request for more suggests it’s eager to maintain the momentum. | Evan Vucci/AP Photo
President Joe Biden’s pledge to “end cancer as we know it” is a rare sliver of common ground between Democrats and Republicans.
Congress has appropriated $1.8 billion for the “cancer moonshot” Biden began in 2016, and the positive reaction to Biden’s request for more during Tuesday’s State of the Union suggests it’s eager to maintain the momentum.
But cancer researchers are less unified about the moonshot than Washington policymakers. A contrarian cadre question whether the money appropriated is being well spent. Cancer research is funded well enough, they said, and investing more in high-tech individualized treatments is more likely to help the wealthy live longer than it is to save those most likely to die of the disease: the poor and people of color.
“It’s a lot harder than getting a man to the moon,” Gilbert Welch, an internist and senior investigator at the Center for Surgery and Public Health at Brigham and Women’s Hospital in Boston, said of curing cancer. “It’s a very complex set of diseases. You need to think of it as a family of diseases. The moon is just one thing. Just gotta get there. This is hundreds of different things.”
Biden wants to press ahead on a bipartisan initiative. He has called on Congress to maintain funding for the 2016 law that launched the moonshot, the 21st Century Cures Act. He pledged to cut cancer death rates by 50 percent in the next 25 years and to turn fatal cancers into treatable diseases.
Biden also has asked Congress to reauthorize the National Cancer Act, signed into law by President Richard Nixon in 1971. Reauthorization would help the National Cancer Institute support researchers around the country by building clinical trial networks and more robust data systems, according to Danielle Carnival, the White House’s moonshot coordinator.
But some experts, such as Ezekiel Emanuel, an oncologist, a professor at the University of Pennsylvania and former White House adviser, said there’s plenty of money devoted to cancer research. The National Cancer Institute had a nearly $6.4 billion budget for cancer research in 2021 and its annual spend has been growing since 2015. Cancer non-profits like the American Cancer Institute also raise hundreds of millions of dollars every year.
President Joe Biden has asked Congress to reauthorize the National Cancer Act, signed into law by President Richard Nixon in 1971. | AP Photo
Additionally, the pharmaceutical industry is incentivized to put money behind increasingly lucrative cancer diagnostics and therapeutics. Research shows that from 2010 to 2019 revenue generated from cancer medicines increased 70 percent among the top 10 pharmaceutical companies to reach $95 billion.
And not everyone thinks more funding is a good thing. “There’s so much money sloshing around,” Welch said of the cancer industry, adding, “Both academic and biotech or industry are excessively enthusiastic and just trying to put out as many products as they can.”
We’ve overinvested in cancer, according to Welch, especially in expensive cancer drugs with modest or unproven benefit for patients and in screenings — Welch’s research area. He’s particularly opposed to the Medicare Multi-Cancer Early Detection Screening Coverage Act, sponsored by Sen. Mike Crapo (R-Idaho) and Rep. Terri Sewell (D-Ala.), which would require Medicare to cover cancer blood tests if they’re approved by the FDA. From Welch’s vantage point, benefits from screenings have been exaggerated, while its harms have been minimized.
Other critics, such as Keith Humphreys, a public health professor at Stanford University who has published academic articles on the link between alcohol use and cancer, see cancer prevention as a more immediate way to save lives.
Managing disease and curing it
The president’s agenda goes beyond money, Carnival told POLITICO, emphasizing prevention efforts, such as improving nutrition for kids, discouraging smoking, and decreasing environmental risks.
“We’re going to have to reach more people with the tools we already have and those we develop along the way,” Carnival said. “The purview is much broader than research. I don’t think anyone would say we have all of the research advancements and knowledge and treatments that we need today to end cancer as we know it.”
Those closely involved in developing cutting-edge cancer therapeutics said the field has shifted dramatically in recent years. It’s gone from treating cancer as a chronic disease, to trying to cure patients.
During his medical fellowship in the early 2000s, improving patient survival by months or years was the goal, explained Marco Davila, a physician-scientist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., who helped pioneer some of the first CAR-T cell therapies for patients with blood cancer.
Since then, treatment breakthroughs for some previously incurable cancer have upended the cancer-as-chronic-disease philosophy. Now, doctors and researchers believe cancer-curing therapies are within reach. “It’s changed the nature of how we manage patients. There’s that option there. It’s on the table,” Davila said.
For Davila, moonshot funds earmarked for cancer research and therapies created a new pool of money for his work. It doesn’t fix the problem of underfunded science as a whole, he said, but it makes his work as a cancer researcher a priority.
“It’s great for us, because that’s our field. It’s also great for patients, because cancer is still going to be one of the most common causes of people’s death in the United States,” Davila said. (In the U.S., it’s second behind heart disease, taking more than 600,000 lives in 2020, the most recent year for which there are statistics.)
Indeed, since the late 1980s, scientists have developed effective treatments for lung cancer, breast cancer and Hodgkin’s lymphoma. There are caveats, of course. They don’t work for all patients.
“It’s maybe 20 percent, 30 percent,” Davila said. The goal now is to keep improving those cure rates over time — to 50 percent or 60 percent, for example.
“Will it get to 100 percent in your lifetime? I don’t know,” he said.
What Davila does know is that each 10 percent cure-rate increase means saving tens of thousands, or even hundreds of thousands of lives.
‘Prevention takes action’
But some cancer experts said there’s a downside to the shift toward precision medicine and individualized treatments. Attempting to test everyone or characterize every tumor more precisely is a bit of magical thinking, according to Welch.
“The more you subset people, the more difficult it is to know whether your treatments help. It’s too small of a group,” Welch said. “It used to be just lung cancer. Now we’ve got eight genetic variants we’re testing in adenocarcinomas of the lung,” he added.
“Ironically, the more precise we get, the more types of cancer there are, as we genetically signature each cancer, all of a sudden we don’t really know what to do with any one of them.”
Others think there needs to be a fundamental shift away from screening and treatment and toward preventing cancer in the first place.
“It’s terrific when we develop new treatments for cancer, but it certainly is always better to prevent something than to treat it,” said Humphreys, who served as a drug policy adviser under Presidents George W. Bush and Barack Obama.
“Very high-end, complicated treatments are never going to be accessible to the whole population,” he added. “Congress could definitely do more.”
“We have very good evidence that when we raise the federal alcohol tax that fewer people die.”
Keith Humphreys, public health professor at Stanford University
Tobacco taxation is widely considered one of the most effective practices in preventing people from starting to smoke in the first place, leading existing smokers to quit, and reducing deaths from tobacco-related cancers. Humphreys said Congress could take the same taxation approach to the alcohol industry. “We have very good evidence that when we raise the federal alcohol tax that fewer people die,” he said.
While broad blood-based cancer screening may not be a cost-effective strategy for stopping cancer early, targeted cancer screening for colorectal, breast, cervical, prostate, and lung cancers could be. Rules could stoke participation or ensure that patients on Medicaid, who are more likely to be at risk of cancer, are getting regular screenings.
“It’s important to acknowledge that our biggest success in cancer really reflects prevention,” Welch said. “It’s nothing fancy. It’s discouraging cigarette smoking.”
There’s a lot of money already in the moonshot cancer system. It just needs to be redirected and allocated differently, said Ezekiel Emanuel, an oncologist and former White House adviser.
The White House touts prevention in its moonshot agenda. In 2022, the first year of the reignited moonshot, the FDA proposed rules to prohibit menthol cigarettes. Among other agenda items, the moonshot program plans to increase cancer screenings in at-risk communities and facilitate donations of sunscreen to schools and youth organizations.
But prevention is a trickier cancer-prevention mechanism than treatment. It could mean cleaning up Superfund sites or removing lead pipes to reduce environmental cancer risk. It often requires people to change their behavior — to drink less alcohol and exercise more or stop smoking — a more challenging mission at the population level than directing patients to take a pill or offering them a diagnostic test.
“It’s not necessarily clear how one spends money on prevention,” Welch acknowledged. “It’s much easier to sell a test or a drug. It’s a concrete thing. Prevention takes action on the part of individuals,” he said. “You gotta say, that’s harder.”
More funding wouldn’t necessarily solve the problem, according to Emanuel.
There’s a lot of money already in the system. It just needs to be redirected and allocated differently, Emanuel explained.
Who is spending that money also matters. The government sponsors roughly one-third of clinical cancer research, according to Emanuel. Industry accounts for the remaining two-thirds of funding. “It’s good that they’ve got a lot of drugs that they’re testing. What’s bad is having industry shape the clinical research agenda, because industry has a bias.”
Emanuel’s solution: stronger government leadership and more non-industry sponsors.
“The NCI [National Cancer Institute] is the biggest NIH institute,” Emanuel said. “It’s not exactly like they’re starving.”
You also have to be a monster to sell halving the cases long after your death as a “cure”
Biden keeps rambling about curing cancer because he and Obama set up and funded the delusional mRNA industry, which was initially aimed at cancer. The Moderna guys promised him this and he ran with it. He still does, poor dumb fv<k…
And if you have a MAGA hat, don’t flash it before reading this:
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
The only thing worse than genocide is irreversibly compromising the human genetics with incalculable consequences for all current and future generations. And, once again, we bring proof they are knowingly doing this, and where there’s awareness, there’s also intention. So this video below should open the Nuremberg 2 trials.
The WEF published this video in 2016, one year prior to Moderna’s Tal Zaks video for TED that we’ve already manage to make quite viral. This crucial issue is hugely underrated and most people still are not so sure what to believe simply because The Military Biotech Complex is burning the books through its Big Tech arm. Hopefully the video before clarifies the issue for good.
Before we further discuss this, please see this “prequel” for very important context:
Actually, one of our first videos deleted by YouTube was just scientists describing their work in the field of epigenetics and epitratrascriptomics, a whole science dedicated to editing DNA using RNA as a screwdriver. See:
Now that we are on the same page, in terms of information, I’d like to go back to our new video, there’s a few key points that I’d like to stress:
They’ve been in the know since Day 1, this is not a surprising side effect, it’s the effect they pursued.
The above implies intention
Obviously they have no clue what this will lead to, other than genetic chaos. In the words of Bill Gates “If you want to see the effects after two years, you need to wait two years”. How about 20 or 200 years?
Cherry on the cake – the newest revelations: 50% truncated mRNA that no one has any clue what it does
All of the above is potentially irreversible, definitive and transmissible to the future generations. We have no clue what’s going to happen, but your grand-grand-grand kids may all suffer from it. Even if you’re a pure blood, you can get contaminated a million ways. AND THAT’S WHAT’S WORSE THEN GENOCIDING A GENERATION IN ONE COUNTRY OR ANOTHER.
Which brings me to another crucial question I launched in the public square long ago, without any satisfactory response:
You all know DNA is described as made of two protein spirals. If you take one and you break it to pieces, the result is hardly different from RNA or their description of a virus. In which case I would love an expert to explain:
What happens to the DNA debris resulted from cell death, where does it go and can it be mistaken for viruses? Are infections and diseases actually auto-immune attacks?
Here’s a possible starting point:
Mechanisms and physiology of the clearance of dead cells by efferocytosis
“Unlike PAMPs, which are derived from microbes, damage-associated molecular patterns (DAMPs) are of cellular origin and can be liberated upon cell death. DAMPs trigger inflammatory responses, and may also serve as chemoattractants for macrophages. DAMPs are metabolically diverse entities, including genomic and mitochondrial DNA, nuclear proteins (HMGB, histones)25, cytoplasmic proteins (S100), cytokines (IL-1α, IL-33, IL-36), and other small molecules (ATP, UTP, uric acid crystals) (Table 1)26. In addition, inflammasome [G] -mediated caspase-1 activation generates inflammatory cytokines IL-1β and IL-18 during pyroptosis (see Box 1) that lead to inflammatory immune activation after cellular demise.27 Below, we review the relevance of DAMPs during efferocytosis, the ability of DAMPs to modulate inflammation, and specific DAMPs and their effects.
DNA as a DAMP.
Several mechanisms ensure low DNA burden following apoptotic death and contribute to its immune-silent phenotype. In healthy cells, caspase-activated DNase (CAD) exists in complex with its inhibitory chaperone ICAD and remains constitutively inactive in the cytosol28,29. Active caspase-3 cleaves ICAD28,30, promoting CAD homodimerization, nuclear translocation, and DNA hydrolysis between nucleosomes. Nuclear pieces are then neatly packaged with cytoplasm into apoptotic bodies that are eventually digested during efferocytosis31. In contrast, nuclear and mitochondrial DNA (mtDNA), as well as pathogen-derived DNA molecules in those cells dying due to an infection, can be released to the extracellular environment from non-apoptotic dying cells. Toll-like receptor 9 (TLR9) is activated by unmethylated CpG sequences such as those found in mtDNA or bacterial DNA (Table 1), and activation of TLR9 triggers downstream inflammatory responses. circulating DNA DAMPs can accumulate in the body in cases where non-apoptotic cell death is widespread; for example, mtDNA was found to be elevated in the plasma of trauma patients32, likely as a result of injury-induced cell death.
DNA in the extracellular environment is processed by DNase-I33, while DNase-III (also known as TREX1) clears cytoplasmic DNA34, and DNase-II processes DNA from dying cells in the phagocyte’s lysosomes to help maintain negligible levels of DNA following efferocytosis. Should DNA escape to the cytosol, it can be recognized by cytosolic DNA sensors35, including cyclic GMP-AMP synthase (cGAS) and the inflammasome component AIM2. cGAS is activated upon cytosolic DNA binding and subsequently catalyzes a reaction between GTP and ATP to form cyclic GMP-AMP (cGAMP)36. The newly synthesized cGAMP binds to and activates the stimulator of interferon genes protein (STING), leading to TANK binding kinase 1 (TBK1)-dependent phosphorylation of the interferon regulatory factor IRF337. These events trigger the IRF3-mediated activation of a Type I interferon response.
DNase-II-deficient or DNase III-deficient mice die during embryogenesis and this embryonic lethality can be prevented if the response to misplaced DNA is abrogated through deletion of cGAS, STING, or the Type-I interferon receptor (IFNAR)38–41. It is possible that these DNases function to limit cytosolic DNA following efferocytosis during development, thereby preventing this lethal interferonopathy, although how the DNA of engulfed corpses might be released from the phagosome or lysosome to become cytosolic, triggering such responses, remains unknown.
Similarly, recognition of cytosolic DNA by AIM2 causes AIM2 to recruit and activate caspase-1, resulting in IL-1β processing and release, contributing to inflammation42,43. Again, when and how defects in the clearance of DNA during efferocytosis may engage AIM2 remains unclear.
Protein DAMPs.
High mobility group protein B1 (HMGB1) is a nuclear protein that binds to DNA and assists replication, repair and transcription44,45,46. Although some HMGB1 can be released to the extracellular milieu under steady state conditions47 or during apoptosis48, it is predominantly released during forms of immunogenic cell death25. Efficient efferocytosis can thus limit the release of HMGB1. Based on its redox status, HMGB1 can function as a chemotactic agent (reduced) or as an inflammatory agent (oxidized)49. In its reduced form, HMGB1 can prevent the induction of immune tolerance [G] to antigens associated with the dying cell48. Reduced HMGB1 may bind to TLRs or the receptor for advanced glycation end products (RAGE) (Table 1)50, leading to immune cell activation and cytokine production. Recently, binding of reduced HMGB1 to the chemokine receptor CXCR4 was observed during tissue regeneration following injury51, highlighting the possible importance of this molecule in the response to dying cells. S100 proteins can also be released from dying cells52, and efferocytosis can limit the release of these proteins from dying cells. Again, TLRs and RAGE appear to be the primary receptors on macrophages that promote inflammatory activation in response to S100 proteins.”
Efferocytosis is critical for tissue homeostasis.Efferocytosis can be carried out by professional phagocytes (red boxes), such as macrophages and dendritic cells, or to a lesser extent by non-professional phagocytes (blue boxes) such as epithelial cells. Disruption of normal efferocytosis can contribute to the development of a wide range of pathologies (light grey boxes) across a variety of tissues. (dark grey boxes). COPD, chronic obstructive pulmonary disease; IPD, idiopathic pulmonary disease; SLE, systemic lupus erythematosus.
I keep my expectations low, but please surprise me!
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Why do we even need science and media investigations, or even a Justice system and police investigators, since YouTube can easily arbiter debates as complex and specific as mRNA technology vs. your genetic code?!
First, please watch the short bombshell video that got scrubbed, as it was uploaded in YouTube too, an unmissable “gem” in itself, even without the censorship scandal :
Here’s a Moderna-produced video for the Moderna website, confirming Moderna’s chief scientist three years later:
Can we cure genetic diseases by rewriting DNA? | David R. Liu – TED 2019
Bonus: TheirTube penalized not only Zaks, but mostly users who followed and spread TheirScience, TheirScientists, TheirAuthoritativeSources
How do I know this? Because I am the one that unearthed this video about two years ago and has worked hard to viralize it. Quite successfully I’d say, it was the most viewed from our channel, I think it was approaching 200,000 views last time I checked, which was a long time ago anyway. But it’s up on other platforms too and other users mirrored it from us, it made several rounds of the Internet and was just blowing up again on Facebook. I’ve seen it deleted multiple times from multiple platforms. So I guess it became too unbearable for the Borg.
NOTICE THAT THE VIDEO THUMBNAIL IS A SCREEN-SHOT OF THE ORIGINAL YOUTUBE UPLOAD, AND THAT’S INTENTIONAL! IT WAS THE SAME HOW I DID IT ON YOUTUBE, SO THEY KNEW WHAT THEY DELETE WHEN THEY DELETED IT. I used another title to bring the video into the 2021 actuality, but kept the original. My title only highlighted another relevant quote from Zaks. This was my one and only intervention in that content.
By the way, I have no control over what’s going on on that channel, because these nitwits deleted my YouTube account completely, for similar crimes, but kept up the orphaned channel.
Btw, this exact scenario happened before, more than once, this is how we lost a few channels and YouTube accounts:
so i can’t even begin to tell you how important it is to spread this info right now, so we can take advantage of the censorship debates and INSERT IN THE PUBLIC AGENDA THE TOPIC of genetic modification by covid jabs!
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
The Internets got agitated recently at the news that Moderna’s CEO, Stephane Bancel, dumped $400Million in Moderna stocks and nuked his Twitter account. Here’s why this shouldn’t surprise you and you should expect the worst any moment now.
Have you watched the former Blackrock director that went on Bannon’s War Room and prophesied that the Covid vaccines are a bubble that’s about to pop? Everything I’ve learned lately stands to support his claim.
If the dumping were a sudden and unusual move, this would indicate a recent event that shook the system, possibly rats leaving a sinking ship, a near threat for the business, as in:
That’s the case only partly, due to the stock crash overlapped with the incoming financial report, but a constant behavior over the span of months and years rather indicate a strategy and it’s associated with insider trading more often than not.
Surprisingly, it’s NPR of all the fakestream media who came in support of my suspicions, with a pretty merciless analysis of Moderna’s leadership financial behavior. And you know what’s funny? The piece dates all the way back to September 2020. I recommend reading the whole piece, I added the bolding and highlights :
Whether the coronavirus vaccine developed by Moderna succeeds or not, executives at the small biotech company have already made tens of millions of dollars by cashing in their stock. An NPR examination of official company disclosures has revealed additional irregularities and potential warning signs.
“On a scale of one to 10, one being less concerned and 10 being the most concerned,” said Daniel Taylor, an associate professor of accounting at the Wharton School, “this is an 11.”
Taylor said Moderna’s stock-selling practices appear well outside the norm, and raise questions about the company’s internal controls to prevent insider trading.
Since January, CEO Stéphane Bancel has sold roughly $40 million worth of Moderna stock held by himself or associated investment funds; Chief Medical Officer Tal Zaks has sold around $60 million; and President Stephen Hoge has sold more than $10 million.
Stéphane Bancel, chief executive officer of Moderna, has sold roughly $40 million worth of stock in the company since the beginning of this year.
The stock sales first came to widespread notice after Moderna announced positive early data from a vaccine trial in May [2020 – S.m.]. At that point, the company’s share price jumped and official disclosures showed executives cashing in their shares for millions of dollars.
“As long as stocks are sold after public announcements – and not before – one might conclude that for an executive with significant net worth tied up in the company, it’s a prudent thing to do,” said Marc Fagel, a former longtime enforcement official with the Securities And Exchange Commission (SEC). “But the optics aren’t great.”
The Moderna vaccine was quick to reach a phase 3 trial, and is seen as a promising contender. But, in some ways, the executives’ stock sales have overshadowed the company’s progress.
Advocates have questioned whether it’s appropriate for executives to privately profit before bringing the vaccine to market, especially when American taxpayers have committed roughly $2.5 billion to the company’s vaccine development and manufacture.
Here’s what NPR’s examination found:
Stock Sales Worth Tens Of Millions: Since June 1, NPR has found, company executives have sold roughly $90 million worth of Moderna stock. Rather than put a hold on the trades after facing intense criticism in May, company executives continued to sell.
Questionable Modifications To Stock Sale Plans: Moderna says its executives pre-scheduled their stock sales long in advance. Those schedules – known as 10b5-1 plans – can act as a defense to charges of insider trading. But the plans have to be put in place when executives do not have confidential inside information. NPR has found multiple executives adopted or modified their plans just before key announcements about the company’s vaccine. That has raised questions about whether they were aware of nonpublic information when they planned their stock trades.
Selling To Zero: Generally, corporate best practices suggest that a company’s leadership should hold on to at least some stock in their company to have “skin in the game.” That way, the thinking goes, an executive has an incentive to improve the company’s performance. As Moderna has been developing its coronavirus vaccine, two executives, including the Chief Medical Officer, have sold all their stock holdings in the company. The General Counsel has sold nearly all of her holdings.
In an interview with NPR, Ray Jordan, Moderna’s Chief Corporate Affairs Officer, said the company has strict internal policies in place to prevent illegal insider trading. For example, Jordan said, the company only allows employees to make changes to their stock sale schedules when they don’t have confidential inside information that could affect the company’s share price.
NPR asked Jordan why Moderna executives modified their 10b5-1 plans just before major announcements. Initially, Jordan said by email, “I believe you must have your dates wrong.”
NPR then provided documentation of those dates from the company’s official disclosures to the government, which Jordan did not dispute.
Jordan then said that even though multiple Moderna executives changed their 10b5-1 plans within one business day of announcements, the company had determined that those executives did not have “material nonpublic information” – a key term for insider trading – when they made those changes.
A spokesperson for the SEC declined to comment for this story.
From a relative unknown, to a key player in the vaccine race
Moderna launched in 2010 with a headquarters based in Cambridge, Mass., focused on using a technology called messenger RNA (or mRNA) to develop vaccines and therapeutics. The mRNA technology has been widely considered innovative, but remains largely unproven. The company has never brought a product to market. In early January, Moderna was trading for under $20 per share, and was valued at around six billion dollars.
Then Moderna announced that it had started collaborating on a coronavirus vaccine with scientists from the National Institute of Allergy and Infectious Diseases, which is led by Dr. Anthony Fauci.
By April, the government had committed half a billion dollars to the Moderna vaccine project as part of Operation Warp Speed.
Since then, the company’s stock price has exploded. Press releases suggesting positive news from the scientific trials, or announcing additional commitments of taxpayer funding sent the share price to a peak of around $95, before dropping to between $60-$70 in recent months. The company is now valued at around $25 billion.
As a result, shares owned by Moderna executives suddenly became much more valuable. And those executives have cashed in tens of millions of dollars worth of stock, according to filings with the SEC.
The bad press and critical comments did not deter continued sales. Since June 1, NPR found, executives sold around $90 million worth of stock.
Public money, private gain
The U.S. government is making massive financial bets on several vaccine candidates. In all likelihood, only some of those vaccine candidates will prove sufficiently safe and effective.
“If the vaccine doesn’t work, you lost a lot of money,” Fauci has said. “But we feel this is serious enough that it’s worth the financial risk.”
But even if taxpayers lose money betting on Moderna, the company’s executives have already made millions.
“The insiders are making plenty of profit and they’re mostly doing it with our money,” said Margarida Jorge, a campaign director with the group Lower Drug Prices Now. “I’m absolutely for deploying public money in the interests of public health and the public good. But we don’t have any commitment from the administration that any of this investment is ultimately going to benefit real people.”
Moderna has argued that the company was only in a position to work with the government on a coronavirus vaccine, because it had spent a decade developing its mRNA technology with the support of private investors.
“The company has been funded over the years by billions of dollars of private investment,” Zaks told the Freakonomics podcast in August. “Those billions created the opportunity for the U.S. government to come in earlier this year and say, ‘I’m going to add some money to the pot to make sure that you get the development for this vaccine right.'”
[But they locked in the Government and its funding for mRNA technology years before SARS-COV2, as shown below, so this was a deliberate lie – S.m]
Trying to resuscitate the company with some archive work?
“Set it and forget it” stock plans
Moderna has offered another defense of those stock sales: the sales, representatives and executives say, were scheduled well in advance, and were unrelated to the market-moving announcements about the coronavirus vaccine. An NPR examination of the company’s financial filings tells a more complicated story.
The schedules are known as 10b5-1 plans. If your stock trades are on autopilot, the idea goes, then you can’t be accused of insider trading. But these “set it and forget it” plans have to be adopted when executives do not have “material nonpublic information,” to use the legal term.
In an interview with CNBC in July, CEO Bancel said he and other executives set up their 10b5-1 plans “a long time ago” – in December 2018 – and “obviously, when we set up those plans, none of us had any idea what was going to happen in 2020.”
In fact, NPR has found, Moderna executives, including Bancel himself, implemented new plans or modified older plans at multiple points in 2020, and right around key announcements related to the company’s vaccine.
On Jan. 21, 2020, for example, Chief Medical Officer Dr. Tal Zaks amended his 10b5-1 plan. (It’s unclear what changes he made.)
Then, on Jan. 22, Moderna first widely confirmed that it was working with the government on a coronavirus vaccine. The following day, Jan. 23, the company announced it had received additional funding to support its coronavirus vaccine development.
NPR asked Moderna whether Zaks might have been aware of the collaboration with the government when he changed his stock trading plan.
“What was known on that particular day or not known, I couldn’t specifically talk to,” Moderna’s Jordan told NPR. But he said that the Moderna legal team only allows employees to change their 10b5-1 plans if they do not possess inside information that could affect the company’s share price.
Later, on Friday, March 13, three Moderna executives adopted new 10b5-1 plans, according to records reviewed by NPR: Zaks, Chief Technical Operations and Quality Officer Juan Andres, and then-Chief Financial Officer Lorence H. Kim. (Kim left the company in August 2020.)
On Monday, March 16 – one business day later – the company announced that it had given a participant the first dose of their vaccine as part of its phase 1 trial. The stock ended that day up 24% compared to the previous day’s close. Moderna was “bucking the trend” of the broader market, which was panicking over coronavirus fears, one CNBC host said at the time.
Timing Of Changes To Pre-Scheduled Stock Sales Raises Questions
Jan. 21 – Chief Medical Officer Dr. Tal Zaks amends his schedule of stock sales, known as a 10b5-1 plan.
Jan. 22 – Moderna widely confirms that it is working on a coronavirus vaccine with the National Institutes of Health. The company’s share price rises nearly 5% over the previous day’s close.
Jan. 23 – Moderna announces new funding from the Coalition for Epidemic Preparedness Innovations.
Mar. 13 – Chief Technical Operations Officer Juan Andres, Chief Financial Officer Lorence Kim, and Zaks adopt new 10b5-1 trading plans.
Mar. 16 – Moderna announces that it provided the first dose of its coronavirus vaccine to a participant in a phase 1 trial. Moderna stock climbs 24% over the previous day’s close.
May 18 – Moderna reports early positive data from its phase 1 trial. The company’s stock ends the day up 20% over the previous day’s close.
May 21 – CEO Stéphane Bancel adopts and amends multiple 10b5-1 trading plans.
May 29 – Moderna announces another milestone in its phase 2 coronavirus vaccine trial.
June 1 – President Stephen Hoge amends his 10b5-1 plan.
Despite the close timing, Jordan told NPR, “by the judgment of the legal team, there would not have been material, nonpublic information known” when executives entered into the new plans.
“Every company and individual is entitled to the presumption of innocence. That said, from the public’s perspective, this trading behavior looks very problematic,” said Taylor of the Wharton School, who first pointed out the timing of these changes to NPR.
“If I put on my SEC enforcement hat, I would certainly be asking, ‘What caused you to change the plan on a Friday?'” said Kurt Wolfe, who works as a defense attorney in securities cases for the firm Troutman Pepper. “I don’t think it’s a good fact pattern.”
On May 21 – in between announcements of major vaccine trial milestones on May 18 and May 29 – CEO Bancel amended and adopted 10b5-1 plans. And on June 1, President Hoge amended his trading plan.
“Amending a trading plan after a positive announcement, like trading after a positive announcement, is only problematic if the executive possesses material, nonpublic information at the time,” said Fagel. “Though repeated or questionably-timed changes to a trading plan will reduce its value as a defense to insider trading.”
Selling to zero
Using these 10b5-1 plans, two Moderna executives – Zaks and Andres – have sold all of their shares in the company. General Counsel Lori Henderson has sold nearly all of her shares.
In fact, roughly every week since June, Zaks has exercised stock options (meaning, he bought stock at a price set by the company as part of his compensation), and then immediately sold all of his shares for a significant profit.
[Isn’t this a great explanation for Bancel’s sales too?! – S.m]
On Aug. 24, for example, Zaks exercised stock options and bought 25,000 shares at bargain prices of between $12 to $21. He then immediately sold all of those shares for around $65 per share. Zaks ended up with a profit of nearly $1.2 million.
SEC filings indicate these trades are made under the 10b5-1 plan he adopted in March.
Selling so much stock can also raise concerns for investors – and the public – about why company leaders would sell now if they expected their vaccine to succeed later. After all, a safe and effective vaccine could send Moderna’s stock to even greater heights.
“It perhaps draws questions about how much they believe in it,” said Wolfe.
If the company does develop a safe and effective coronavirus vaccine, and its stock keeps rising, then “these trades will be water under the bridge,” said Fagel, the former SEC enforcement official.
But, Fagel warns, if the vaccine fails, then SEC regulators and angry investors may come looking for answers. In that case, he said, “both class action litigation and an SEC investigation would seem inevitable.”
NPR revelations end here, we’re actually just starting
So what we’ve learned is that Moderna looks like a stock market operation more than a medical one. The chiefs create momentums and then trade. And they use public money to bet and make billions, but more about that shortly.
This news is actually pretext to get you to know the real history of Moderna, a crux point in modern history in the widest sense. The stock dumping is not really news, it’s been happening for quite a while, indicating a long term strategy and business model, rather than a sudden or impulse move.
The next two older reports from Pharma’s own media – STAT, will cement the certainty that Moderna turned into a stock market bubble long ago, under the helms of Stephan Bancel. They don’t mind having some science to show, but that’s just the bait.
Ego, ambition, and turmoil: Inside one of biotech’s most secretive startups
At first glance, Moderna Therapeutics looks like the most enviable biotech startup in the world. It has smashed fundraising records and teamed up with pharmaceutical giants as it pursues a radical plan to revolutionize medicine by transforming human cells into drug factories.
But the reality is more complicated.
A STAT investigation found that the company’s caustic work environment has for years driven away top talent and that behind its obsession with secrecy, there are signs Moderna has run into roadblocks with its most ambitious projects.
At the center of it all is Stéphane Bancel, a first-time biotech CEO with an unwavering belief that Moderna’s science will work — and that employees who don’t “live the mission” have no place in the company. Confident and intense, Bancel told STAT that Moderna’s science is on track and, when it is finally made public, that it will meet the brash goal he himself has set: The new drugs will change the world.
But interviews with more than 20 current and former employees and associates suggest Bancel has hampered progress at Moderna because of his ego, his need to assert control and his impatience with the setbacks that are an inevitable part of science. Moderna is worth more than any other private biotech in the US, and former employees said they felt that Bancel prized the company’s ever-increasing valuation, now approaching $5 billion, over its science.
As he pursued a complex and risky strategy for drug development, Bancel built a culture of recrimination at Moderna, former employees said. Failed experiments have been met with reprimands and even on-the-spot firings. They recalled abusive emails, dressings down at company meetings, exceedingly long hours, and unexplained terminations.
At least a dozen highly placed executives have quit in the past four years, including heads of finance, technology, manufacturing, and science. In just the past 12 months, respected leaders of Moderna’s cancer and rare disease programs both resigned, even though the company’s remarkable fundraising had put ample resources at their disposal. Each had been at the company less than 18 months, and the positions have yet to be filled.
Lower-ranking employees, meanwhile, said they’ve been disappointed and confused by Moderna’s pivot to less ambitious — and less transformative — treatments. Moderna has pushed off projects meant to upend the drug industry to focus first on the less daunting (and most likely, far less lucrative) field of vaccines — though it is years behind competitors in that arena.
The company has published no data supporting its vaunted technology, and it’s so secretive that some job candidates have to sign nondisclosure agreements before they come in to interview. Outside venture capitalists said Moderna has so many investors clamoring to get in that it can afford to turn away any who ask too many questions. Some small players have been given only a peek at Moderna’s data before committing millions to the company, according to people familiar with the matter.
“It’s a case of the emperor’s new clothes,” said a former Moderna scientist. “They’re running an investment firm, and then hopefully it also develops a drug that’s successful.”
Like many employees and former employees, the scientist requested anonymity because of a nondisclosure agreement. Others would not permit their names to be published out of fear that speaking candidly about big players in the industry would hurt their job prospects down the road.
Moderna just moved its first two potential treatments — both vaccines — into human trials. In keeping with the culture of secrecy, though, executives won’t say which diseases the vaccines target, and they have not listed the studies on the public federal registry, ClinicalTrials.gov. Listing is optional for Phase 1 trials, which are meant to determine if a drug is safe, but most companies voluntarily disclose their work.
Investors say it’ll be worth the wait when the company finally lifts the veil.
“We think that when the world does get to see Moderna, they’re going to see something far larger in its scope than anybody’s seen before,” said Peter Kolchinsky, whose RA Capital Management owns a stake in the company.
The Moderna offices in Cambridge, Mass.ARAM BOGHOSIAN FOR STAT
Bancel, meanwhile, said he is aware of the criticism of him and has taken some steps to address it. After scathing anonymous comments about Moderna’s management began showing up online, Bancel went to Silicon Valley to get tips on employee retention from the human resources departments of Facebook, Google, and Netflix. But he makes no apologies for tumult past or present, pointing to the thousands of patients who might be saved by Moderna’s technology.
“You want to be the guy who’s going to fail them? I don’t,” he said in an interview from his glassy third-floor office. “So was it an intense place? It was. And do I feel sorry about it? No.”
An ambitious CEO dreams big
Bancel, 44, had no experience running a drug development operation when one of biotech’s most successful venture capitalists tapped him to lead Moderna. He’d spent most of his career in sales and operations, not science.
But he had made no secret of his ambition.
A native of France, Bancel earned a master’s in chemical engineering from the University of Minnesota and an MBA from Harvard in 2000. As Harvard Business School classmates rushed to cash in on the dot-com boom, Bancel laid out a plan to play “chess, not checkers.”
“I was always thinking, one day, somebody will have to make a decision about me getting a CEO job,” he told an audience at his alma mater in April. “… How do I make sure I’m not the bridesmaid? How do I make sure that I’m not always the person who’s almost selected but doesn’t get the role?”
He went into sales and rose through the operational ranks at pharmaceutical giant Eli Lilly, eventually leading the company’s Belgian operation. And in 2007, at just 34, he achieved his goal, stepping in as CEO of the French diagnostics firm bioMérieux, which employs roughly 6,000 people.
The company improved its margins under Bancel’s tenure, and he developed a reputation as a stern manager who got results, according to an equities analyst who covered bioMérieux at the time.
“He doesn’t suffer fools lightly,” the analyst said, speaking on condition of anonymity to comply with company policy. “I think if you’re underperforming, you’ll probably find yourself looking for another job.”
Bancel’s rise caught the eye of the biotech investment firm Flagship Ventures, based here in Cambridge. Flagship CEO Noubar Afeyan repeatedly tried to entice him to take over one of the firm’s many startups, Bancel said. But he rejected one prospect after another because the startups seemed too narrow in scope.
Moderna was different.
The company’s core idea was seductively simple: cut out the middleman in biotech.
For decades, companies have endeavored to craft better and better protein therapies, leading to new treatments for cancer, autoimmune disorders, and rare diseases. Such therapies are costly to produce and have many limitations, but they’ve given rise to a multibillion-dollar industry. The anti-inflammatory Humira, the world’s top drug at $14 billion in sales a year, is a shining example of protein therapy.
Moderna’s technology promised to subvert the whole field, creating therapeutic proteins inside the body instead of in manufacturing plants. The key: harnessing messenger RNA, or mRNA.
In nature, mRNA molecules function like recipe books, directing cellular machinery to make specific proteins. Moderna believes it can play that system to its advantage by using synthetic mRNA to compel cells to produce whichever proteins it chooses. In effect, the mRNA would turn cells into tiny drug factories.
It’s highly risky. Big pharma companies had tried similar work and abandoned it because it’s exceedingly hard to get RNA into cells without triggering nasty side effects. But if Moderna can get it to work, the process could be used to treat scores of diseases, including cancers and rare diseases that can be death sentences for children.
Bancel was intrigued. He knew it was a gamble, he told STAT, “but if I don’t do it, and it works, I’m just going to kick myself every morning.”
And so he became the company’s CEO — and soon developed an almost messianic reverence for the mRNA technology.
Despite having never worked with RNA before, Bancel said he sat around the table with his core team in the early days of the company, dreaming up experiments. As a result, he is listed as a co-inventor on more than 100 of Moderna’s early patent applications, unusual for a CEO who is not a PhD scientist.
Lavishly funded Moderna hits safety problems in bold bid to revolutionize medicine
SAN FRANCISCO — Moderna Therapeutics, the most highly valued private company in biotech, has run into troubling safety problems with its most ambitious therapy, STAT has learned — and is now banking on a mysterious new technology to keep afloat its brash promise of reinventing modern medicine.
Exactly one year ago, Moderna CEO Stéphane Bancel talked up his company’s “unbelievable” future before a standing-room-only crowd at the annual J.P. Morgan Healthcare Conference here. He promised that Moderna’s treatment for a rare and debilitating disease known as Crigler-Najjar syndrome, developed alongside biotech giant Alexion Pharmaceuticals, would enter human trials in 2016.
It was to be the first therapy using audacious new technology that Bancel promised would yield dozens of drugs in the coming decade.
But the Crigler-Najjar treatment has been indefinitely delayed, an Alexion spokeswoman told STAT. It never proved safe enough to test in humans, according to several former Moderna employees and collaborators who worked closely on the project. Unable to press forward with that technology, Moderna has had to focus instead on developing a handful of vaccines, turning to a less lucrative field that might not justify the company’s nearly $5 billion valuation.
“It’s all vaccines right now, and vaccines are a loss-leader,” said one former Moderna manager. “Moderna right now is a multibillion-dollar vaccines company, and I don’t see how that holds up.”
Bancel made no mention of the Crigler-Najjar drug when he spoke Monday before a similarly packed room at this year’s J.P. Morgan conference.
His presentation instead focused on four vaccines that the company is moving through the first phase of clinical trials: two target strains of influenza, a third is for Zika virus, and the fourth remains a secret. Bancel clicked through graphs of data from animal studies before hurrying on to tout Moderna’s balance sheet and discuss the company’s cancer vaccines, slated for clinical testing later this year.
When STAT asked Bancel after the presentation about Crigler-Najjar, he deferred to Alexion.
In need of a Hail Mary
Founded in 2012, Moderna reached unicorn status — a $1 billion valuation — in just two years, faster than Uber, Dropbox, and Lyft, according to CB Insights. The company’s premise: Using custom-built strands of messenger RNA, known as mRNA, it aims to turn the body’s cells into ad hoc drug factories, compelling them to produce the proteins needed to treat a wide variety of diseases.
But mRNA is a tricky technology. Several major pharmaceutical companies have tried and abandoned the idea, struggling to get mRNA into cells without triggering nasty side effects.
Bancel has repeatedly promised that Moderna’s new therapies will change the world, but the company has refused to publish any data on its mRNA vehicles, sparking skepticism from some scientists and a chiding from the editors of Nature.
The indefinite delay on the Crigler-Najjar project signals persistent and troubling safety concerns for any mRNA treatment that needs to be delivered in multiple doses, covering almost everything that isn’t a vaccine, former employees and collaborators said.
The company did disclose a new technology on Monday that it says will more safely deliver mRNA. It’s called V1GL. Last month, Bancel told Forbes about another new technology, N1GL.
But in neither case has the company provided any details. And that lack of specificity has inevitably raised questions.
Three former employees and collaborators close to the process said Moderna was always toiling away on new delivery technologies in hopes of hitting on something safer than what it had. (Even Bancel has acknowledged, in an interview with Forbes, that the delivery method used in Moderna’s first vaccines “was not very good.”)
Are N1GL and V1GL better? The company has produced no data to answer that question. When STAT asked about new technologies, Bancel referred questions to the company’s patent filings.
The three former employees and collaborators said they believe N1GL and V1GL are either very recent discoveries, just in the earliest stages of testing — or else new names slapped on technologies Moderna has owned for years.
“[The technology] would have to be a miraculous, Hail Mary sort of save for them to get to where they need to be on their timelines,” one former employee said. “Either [Bancel] is extremely confident that it’s going to work, or he’s getting kind of jittery that with a lack of progress he needs to put something out there.”
Former employees and collaborators who spoke with STAT requested anonymity because they had signed nondisclosure agreements — which the highly secretive Moderna requires even some job candidates to sign.
A STAT investigation last year found that Bancel had driven away top talent from Moderna with a culture of recrimination and a caustic work environment, including on-the-spot firings for failed experiments.
The company, based in Cambridge, Mass., seems to have repaired its reputation among many rank-and-file employees, winning workplace accolades from Science Magazine and the Boston Globe, but Moderna has lost more than a dozen top scientists and managers in the past four years, despite its vast financial resources.
A bug in the software
Bancel, a first-time biotech CEO, has dismissed questions about Moderna’s potential. He describes mRNA as a simple way to develop treatments for scores of ailments. As he told STAT over the summer, “mRNA is like software: You can just turn the crank and get a lot of products going into development.”
It seems clear, however, that the software has run into bugs.
Patients with Crigler-Najjar are missing a key liver enzyme needed to break down bilirubin, a yellowish substance that crops up in the body as old red blood cells break down. Without that enzyme, bilirubin proliferates in the blood, leading to jaundice, muscle degeneration, and even brain damage.
In Moderna’s eyes, the one-in-million disease looked like an ideal candidate for mRNA therapy. The company crafted a string of mRNA that would encode for the missing enzyme, believing it had hit upon an excellent starting point to prove technology could be used to treat rare diseases.
But things gradually came apart last year.
Every drug has what’s called a therapeutic window, the scientific sweet spot where a treatment is powerful enough to have an effect on a disease but not so strong as to put patients at too much risk. For mRNA, that has proved elusive.
Before COVID-19, the company’s secretive nature, and its failure to deliver a functional product, was drawing comparisons to the infamous biotech startup Theranos. Similar to Moderna, Theranos rarely published any peer-reviewed material. Like Moderna, Theranos mastered the networking game, and recruited high profile individuals to its board in order to vouch for the company’s “revolutionary technologies.” Once valued at well over $10 Billion, Theranos collapsed after it was revealed that the company was running a massive fraud scheme, in addition to its failure to implement its promised blood testing technology.
“Now an obscure lawsuit filed in British Columbia in October sheds light on one of Moderna’s key partners, and through it FORBES can reveal details on Moderna’s amazing but still untested technology.
It appears that the first two products Moderna has entered into clinical trials rely on technology from a small outfit in Vancouver, British Columbia, called Acuitas Therapeutics. (Acuitas is so small, in fact, that its worldwide headquarters are in its CEO’s single-family home.)
Almost all medicines either block proteins–the building blocks of life–or, in the case of expensive biotech drugs, are proteins themselves. But Moderna has been promising to hack an entirely different part of life’s cookbook. In order to turn genetic information encoded in DNA into the cellular machines that actually are proteins, living things use a messenger chemical called mRNA.
Creating these mRNA drugs is a big challenge on many levels. For them to work, Moderna needs to deliver mRNA to the body’s cells. By itself mRNA breaks down in the bloodstream. Tiny Acuitas specializes in one method: lipid-nanoparticle delivery systems. Its technology essentially wraps the mRNA into balls of fat that disguise the drug so that the target cells will readily ingest it.
“Although we are small,” says Thomas Madden, chief executive of Acuitas, “I believe the technology we have developed is highly effective.”
The problem for Madden and Moderna is that Acuitas doesn’t actually own the technology it has licensed to Moderna. The tech belongs to a third company, publicly traded Arbutus, which recently decided to terminate the license for the tech that it had granted to Acuitas. That’s why Acuitas filed the lawsuit in British Columbia, to protect the deal it had. Arbutus immediately countersued, claiming its deal with Acuitas didn’t cover Moderna’s medicines.
The legal mess has its roots in Moderna’s 2011 start, when Robert Langer, an MIT professor, Moderna board member and founder of dozens of biotech companies, told Bancel that Moderna was too underfunded and small to create its own delivery system. So Moderna vetted over a dozen external delivery methods for mRNA and settled on at least three. One belonged to Arbutus, but Moderna turned to tiny Acuitas to get access to it.
Acuitas was formed in 2009 by Madden after a merger eliminated his position at Arbutus’ predecessor, Tekmira Pharmaceuticals. After a contentious lawsuit Madden was able to license from his former employer the novel tech he had helped develop, and Bancel claims Moderna chose to work with Acuitas because it had “the people and the capabilities.”
But that doesn’t explain why Moderna–flush with capital–didn’t make sure that sublicensing through Acuitas would be okay with Arbutus before advancing its new drugs into human studies.
Bancel met with FORBES at a Brooklyn coffee shop on a recent Saturday to dispel the implications of the lawsuit. He is dismissive of Acuitas’ technology. “We knew it was not very good,” he says. “It was just okay.”
He further explains that Moderna is in the process of producing its own nanoparticle lipids. One such lipid, N1GEL (called “Nigel” internally), appears to cause less inflammation than Acuitas’ version. Another is being licensed from Merck. Bancel says Moderna has stopped using the Acuitas tech for new drugs.
That still leaves a somewhat messy situation for any Moderna vaccines that are being developed using Acuitas’ tech.
Data from one vaccine is expected early next year. If results are good, it could lead to a sizzling-hot initial public offering, even if the Canadian lawsuit ultimately affords Arbutus bigger royalty payments from Moderna.”
Well, the two tiny Canadian companies mentioned above bring royalties to the Canada’s treasury (should I say The British Crown?), so don’t expect Trudeau to backpedal too soon
AND IF ONLY THEY HUSSLED WITH PRIVATE FUNDS, AS THEY CLAIMED…
Moderna chief keep claiming that they started to use public funds only as a patch on infrastructure, science and funding they’ve built for years.
Wrong!
It’s known that NIH + NIAID have long been one of their main sources for the “lavish funding” mentioned earlier and when they locked in the government support, they actually started to leverage it and attract even more private funds, in an self-feeding loop that created today’s monster-bubble.
Very few people know they even got money from BARDA and DARPA. As in “military funds”.
Remember this lie from earlier? “The company has been funded over the years by billions of dollars of private investment,” Zaks told the Freakonomics podcast in August. “Those billions created the opportunity for the U.S. government to come in earlier this year and say, ‘I’m going to add some money to the pot to make sure that you get the development for this vaccine right.'” Watch this claim getting nuked:
This grid above looks familiar to you? It does to me, but it’s not blood from people who underwent Covid genetic therapies, just something similar. Taken from:
KEI asks DOD to investigate failure to disclose DARPA funding in Moderna patents
by Knowledge Ecology International (KEI)
Luis Gil Abinader has taken a deep dive into Moderna’s surprising practice of never declaring government funding in its 126 patents and 154 patent applications, despite having had funding from multiple federal agencies.
One outcome of his research is a 25 page report (RN-2020-3) on Moderna’s failure to report funding from DARPA, and a request by KEI to DOD and DARPA to remedy this, including by taking title to patents where disclosures should have been made. (Text of letter below, and PDF version here).
KEI will also send a letter to BARDA. The letter below was addressed to DOD and DARPA, and focuses on their funding.
Context
The obligation to disclose federal funding in patent applications has been subject to presidential executive orders, statutes, regulations and contracts, including those cited and quoted in Abinader’s report. The disclosure clarifies the public’s rights in the inventions and the obligations on the entity getting the money, on everything from the government’s worldwide royalty free license to the public’s march-in rights, obligations to make inventions available to the public on reasonable terms, and additional safeguards that can be exercised by a government inclined to do so.
Secondly, the disclosure changes the narrative about who has financed the inventive activity, often the most risky part of development.
One of the earlier norms on this was Franklin Roosevelt’s Executive Order 9424, on the Establishment of a Register of Government interests in patents.
In 2018, the regulations on disclosure were modified by NIST (see 83 FR 15954), where, among other things, the government gave itself unlimited time to remedy a failure to disclose federal funding, to eliminate one loophole that created an incentive ignore the disclosure requirement.
In the past, the US Department of Defense has taken title to patents where federal funding was not disclosed. See: Campbell Plastics v. Brownlee, 389 F.3d 1243 (Fed. Cir. 2004).
The research on the Moderna/DARPA funding is outlined in a 25 page August 27, 2020 report by Luis Gil Abinader, titled: “Moderna failures to disclose DARPA funding in patented inventions.” RN-2020-3
Below is the text of the KEI letter to Dr. Mark T. Esper, Secretary of Defense, and Dr. Amy Jenkins, of the Pandemic Prevention Platform for the Defense Advanced Research Projects Agency (DARPA), regarding the apparent failure by Moderna to disclose DARPA funding in patent applications. PDF copy here:
2020. September 18. DARPA letter to KEI confirming investigation of Moderna for failure to report government funding in patent applications. https://www.keionline.org/33970
2020. September 4. BARDA is investigating Moderna’s failures to disclose BARDA funding in patent applications. https://www.keionline.org/33907
2020. September 2. KEI request to BARDA concerning Moderna obligations to disclose federal funding in patent applications. https://www.keionline.org/33892
2020. August 30. DARPA announces investigation into Moderna’s apparent failures to disclose mRNA vaccine patents. https://www.keionline.org/33832
2020. August 28. KEI asks DOD to investigate failure to disclose DARPA funding in Moderna patents. https://www.keionline.org/33763
2020. August 27. 2020:3 KEI Research Note: Moderna failures to disclose DARPA funding in patented inventions. https://www.keionline.org/rn-2020-3
2020. August 5. BARDA Responds to KEI, Public Citizen Letter Asking BARDA to Enforce Moderna Contract. https://www.keionline.org/33633
2020. August 4. KEI and Public Citizen request BARDA to address Moderna’s noncompliance with COVID-19 vaccine contract term. https://www.keionline.org/33618
2020. July 1. KEI receives seven new contracts for COVID 19 research from BARDA and DOD, including five using “Other Transactions Authority” that weaken or eliminate Bayh-Dole and FAR Safeguards. https://www.keionline.org/covid19-ota-contracts
Washington Post 2020. August 28. “Moderna failed to disclose federal support in vaccine patents, researchers say: The company with a leading coronavirus vaccine candidate did not adhere to a law designed to protect public investment.” Washington Post. Christopher Rowland. https://www.washingtonpost.com/business/2020/08/28/moderna-vaccine-patents-darpa-funding/
Financial Times 2020. August 29. “US government’s Darpa probes Moderna’s vaccine patents: Researchers accuse biotech company of failing to disclose federal grants in patents which also cover Covid-19 candidate.” Financial Times. Donato Paolo Mancini. https://www.ft.com/content/2be1f87e-9e96-4e23-9cc5-33ba35e50586
Moderna’s vaccine was developed with support from the NIAID, and, as covered in a past fact check, analysis from Axios found that the National Institutes of Health, of which the NIAID is part, may own intellectual property used in producing Moderna’s vaccine. Dr. Francis Collins, director of NIH, has also said that NIH has a stake in intellectual property used in the vaccine, though what exactly this means in practical terms is unclear.
“Valera’s efforts (Moderna subsidiary) have resulted in the demonstration of preclinical efficacy of Moderna’s mRNA-based vaccines in multiple viral disease models, Moderna said.
In the partnership with the Gates Foundation, Valera will apply its mRNA vaccine platform as well as Moderna’s drug platform Messenger RNA Therapeutics™. Designed to produces human proteins, antibodies, and entirely novel protein constructs inside patient cells, the therapeutics are secreted or active intracellularly.” – Genetic Engineering & Biotechnology News
To avoid a conflict of interest, Slaoui resigned from the board of the Massachusetts-based biotech firm Moderna, which had been developing a vaccine for the coronavirus. He stepped down but he didn’t give up his stakes in Moderna, as the Daily Beast reports:
“Slaoui’s ownership of 156,000 Moderna stock options, disclosed in required federal financial filings, sparked concerns about a conflict of interest. Democratic Massachusetts Senator Elizabeth Warren called Slaoui out over the matter on Twitter: “It is a huge conflict of interest for the White House’s new vaccine czar to own $10 million of stock in a company receiving government funding to develop a COVID-19 vaccine. Dr. Slaoui should divest immediately.” The company’s shares skyrocketed last month after news broke of the $483 million in federal funding to work on a coronavirus vaccine. Slaoui could not immediately be reached for comment on the matter.”
Slaoui also sits on the boards of SutroVax, the Biotechnology Innovation Organization, the International AIDS Vaccine Initiative, and the PhRMA Foundation
So this has never been about health, just a global scale racketeering operation that’s coming to light about about to go bust. You can speed up this process simply by spreading this expose far and wide!
UPDATE MARCH 21, 2022: VOILA!
Via our ex-BlackRock friend Edward Dowd. I rest my case, but I bet they will “unrest” it soon.
Both Pfizer+Moderna have issued huge 2022 revenue guidance to Wall Street for C-19 vaccines: combined nearly 3 billion doses & ~$50b in revenue.
But mRNA demand has waned.
If they don't sell 4th doses, they may need to break their promises to Wall St. and lower their guidance. pic.twitter.com/K0HMdfFBPu
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Stupidity leads to inflated ego, which leads to bragging and ruining months and months of brainwashing efforts from The Great Reset Politburo.
UPDATE: THIS VIDEO LED TO THE DELETION OF OUR THIRD YOUTUBE CHANNEL, EVEN THOUGH IT’S SOURCED FROM YOUTUBE AND THEIR TOP AUTHORITATIVE SOURCES!
ORIGINAL 2H VIDEO:
We all knew this, but it’s good to have it on video from this inbred horse’s mouth. The funny part is that the Covidiocracy is already in panic mode, writing the most inane ‘debunks’, which can be, for the largest part, summed up as “you didn’t hear what you’ve just heard, you heard what we tell you you heard”. They’re literally trying to do Jedi mind tricks on us and I bet there’s weakminded Pharma-junkies out there that will fall for their potato-grade hypnosis.
I can’t stress enough that 95% figure and how easy it was to crash it.
Stefan Oelrich, president of Bayer’s Pharmaceuticals Division and membr of the Bayer/Monsanto board, made these statements at the 2021 World Health Summit in Berlin. on October 24th.
Informed consent had the fate of an Epstein sex slave buried on his island. No one is even looking for it. Without it, the whole Covidiocracy is just genocide and war crimes, covidiots’ masks are soaked in blood, and their survival now depends entirely on the mass ignorance. While ours depends on mass-enlightenment.
Silview ‘SILVIEW’ Costinescu
There’s not much to add, if you want to learn more about Bayer’s dark past, suffice to say they made Zyklon-B, the gas allegedly used in the nazi camps, and more recently have acquired Monsanto. After that, they’ve become more discrete, but they still have their hands in everything that feeds you and everything that treats the diseases you got from their food and their pesticides. And, of course, they’re top tier members of Klaus Schwab’s World Economic Forum, at the forefront of transhumanism and The Fourth Industrial Revolution. But here’s more info:
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
“The latest widest news in Molecular Microbiology”, according to microbiologists. Not so much outside their world. The consequences are beyond imagination…
Here’s the study, my brief comments after:
SARS–CoV–2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro
Severe acute respiratory syndrome coronavirus 2 (SARS–CoV–2) has led to the coronavirus disease 2019 (COVID–19) pandemic, severely affecting public health and the global economy. Adaptive immunity plays a crucial role in fighting against SARS–CoV–2 infection and directly influences the clinical outcomes of patients. Clinical studies have indicated that patients with severe COVID–19 exhibit delayed and weak adaptive immune responses; however, the mechanism by which SARS–CoV–2 impedes adaptive immunity remains unclear. Here, by using an in vitro cell line, we report that the SARS–CoV–2 spike protein significantly inhibits DNA damage repair, which is required for effective V(D)J recombination in adaptive immunity. Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site. Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines. View Full-Text
The study is in vitro (of course), remains to be confirmed in vivo (that will be a long adventure), but it’s very worrying nevertheless.
Some scientists have quickly reacted by demanding a reformulation of the Covid vaccines so that they contain only a fragment of the protein that would delivere the desired effect without the unwanted ones. But: 1) do they have any proof a fragment won’t wreck havoc too? 2) have they forgotten already that the spike originates in the ‘virus’, are they really telling us everyone who had Covid is potentially ‘broken’, or 3) do they think, as I do, that the virus exists only on servers and the protein only in the goo they sell as ‘Covid vaccines’?
Dr Mikolaj Raszek, Phd from Merogenomics
“Antibody Dependent Enhancement or ADE could occur with use of full length of Spike protein”, dr. Rszek says, I’d ask what are the chances for it to NOT occur in the billion people or so that have been chemically raped so far?
What all this involves:
Anyone who got the spike can break down at any time in ways we can’t even fully anticipate. That includes those who got it from a virus as well as those who got it from an injection. Recent discovery that Spikes may circulate for months on end in Exosomes to different parts of the body and in theory enter cells well after the point of vaccination
I’m personally not worried about any natural coronaviruses ever, but if you are or if you think an artificial virus had a pandemic outbreak recently, and it became unescapable, then this is an extinction level threat and the countdown has already started. Reformulating vaccines will only prevent us from pouring gas on our own burning roof.
Whether if you think the spike only comes from the syringe and the shedding vaxxtards, like I do, or from viral sources, vaccination must be stopped NOW, there’s no way the benefits can outweigh the risks!
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Sometimes my memes are 3D. And you can own them. Or send them to someone. You can even eat some of them. CLICK HERE
THERE’S NO BETTER PREVENTION THAN SHARING THE KNOWLEDGE FASTER THAN THEY SHARE THEIR PROPAGANDA!
The original title of this article was URGENT! DEBUNKING THE NEXT ENGINEERED PANDEMIC: NIPAH VIRUS. I expanded the scope because in the meantime I learned they are ramping up propaganda for all three. These viruses have more things in common, as you will find out below.
You should actually begin with this earlier report:
To further develop the ChAd3 Ebola and Marburg vaccines, Sabin has entered into a Research Collaboration Agreement with the Vaccine Research Center at the National Institute of Allergy and Infectious Diseases. The Sabin Vaccine Institute, a non-profit organization founded in 1993, is a leading advocate for expanding vaccine access and uptake globally, advancing vaccine research and development, and amplifying vaccine knowledge and innovation. Sabin received more than $110 million for vaccine R&D programs from public and philanthropic funding sources, including the Bill & Melinda Gates Foundation, European Commission, Dutch Ministry of Foreign Affairs, Global Health Innovative Technology Fund and the Michelson Medical Research Foundation.
Washington DC, Oct. 21, 2021 (GLOBE NEWSWIRE) — The Sabin Vaccine Institute (Sabin) announced that the Biomedical Advanced Research and Development Authority (BARDA), part of the Office of the Assistant Secretary for Preparedness and Response within the U.S. Department of Health and Human Services, has exercised the third contract option, valued at $34.5 million, under the 2019 contract to advance the development of vaccines against Ebola Sudan and Marburg viruses through Phase 2 clinical trials.
In September 2019, BARDA awarded Sabin a development contract, valued up to $128 million, and has already provided funding of $40.5 million. This third contract option will enable continued nonclinical efficacy and safety studies, Phase 2 clinical trials in Africa, and vaccine manufacturing processes to ensure quality and safety.
In August, a case of Marburg disease was confirmed in the West African country of Guinea where the Ministry of Health officially declared an outbreak of Marburg.1 This recent case, as well as Marburg’s history of outbreaks and their potential for future devastating outbreaks, demonstrates that preventative measures are overdue to protect civilian populations, military personnel, first responders, health care workers and laboratory workers, both in the United States and abroad, against these emerging infectious diseases.
Ebola Sudan and Marburg viruses are closely related to Ebola Zaire virus, which has caused more than 2,200 deaths since 2018, leading the World Health Organization (WHO) to declare it a Public Health Emergency of International Concern. Like Ebola Zaire, Ebola Sudan and Marburg are among the world’s deadliest viruses, causing hemorrhagic fever with subsequent death in an average of 50 percent of cases.2,3
“Even as the world struggles with the COVID-19 pandemic, disease caused by Ebola Sudan and Marburg viruses continue to be a serious threat, as we have seen with the recent outbreak of Marburg in Guinea. We are grateful for BARDA’s continued support of Sabin’s efforts to advance vaccines against these deadly viruses,” said Sabin Chief Executive Officer Amy Finan. “We also thank our partners at the Vaccine Research Center of the NIH National Institute of Allergy and Infectious Diseases for their continued collaboration, and GSK for their earlier work on the candidates.”
The two candidate vaccines, based on GSK’s proprietary ChAd3 platform, were exclusively licensed to the Sabin Vaccine Institute from GSK in 2019.
This project has been funded in whole or in part with federal funds from the U.S. Department of Health and Human Services; Office of the Assistant Secretary for Preparedness and Response; Biomedical Advanced Research and Development Authority, under contract number 75A50119C00055.
This above is the official Sabin Inst. press release, this below isn’t:
November 4, 2021 – The U.S. CDC published a Level Three Travel Advisory for the recent Ebola outbreak in the Beni Health Zone of the Democratic Republic of the Congo.
November 3, 2021 – The U.S. CDC vaccine advisory committee reviewed previous recommendation preexposure vaccination with Ervebo for adults aged ≥18 years in the U.S. population who are at highest risk for potential occupational exposure to Ebola virus species Zaire ebolavirus because they are: responding to an outbreak of Ebola Virus Disease (EVD), or work as health care personnel at federally designated Ebola treatment centers in the U.S., or work as laboratorians or other staff at biosafety level 4 facilities in the U.S.
November 2, 2021 – The WHO reported additional cases and deaths confirmed in the Ebola virus disease outbreak in the Democratic Republic of the Congo with two new health areas affected. A total of 394 people (67 primary care providers including nine high-risk contacts, nine contacts of contacts, and 49 probable contacts) have been vaccinated including 182 contacts of contacts, 125 probable contacts, and 87 high-risk contacts.
October 29, 2021 – A Research Article – Safety and immunogenicity of 2-dose heterologous Ad26.ZEBOV, MVA-BN-Filo Ebola vaccination in healthy and HIV-infected adults: A randomized, placebo-controlled Phase II clinical trial in Africa – was published by the journal PLOS Medicine. Conclusion – The Ad26.ZEBOV and MVA-BN-Filo combo vaccination were well tolerated and immunogenic in healthy and HIV-infected African adults. Increasing the interval between vaccinations from 28 to 56 days improved the magnitude of humoral immune responses. Antibody levels persisted to at least 1 year, and an Ad26.ZEBOV booster vaccination demonstrated the presence of vaccination-induced immune memory. These data supported the approval by the European Union for prophylaxis against EBOV disease in adults and children ≥1 year of age.
October 27, 2021 – IAVI announced an award of up to US$126 million from the Biomedical Advanced Research and Development Authority to develop two recombinant vesicular stomatitis virus (rVSV)-vectored filovirus vaccine candidates. This award supports preclinical activities and includes options for clinical development up to and inclusive of a Phase II clinical trial of IAVI’s rVSV Sudan ebolavirus vaccine candidate (rVSVΔG-SUDV-GP). Optional work that would continue the development of IAVI’s Marburg virus vaccine candidate (rVSVΔG-MARV-GP) that is currently supported by the Defense Threat Reduction Agency of the U.S. Department of Defense could be funded at a later date.
“Vectored” means, most likely, mRNA or some other genetic / nanotech targeting technology.
October 20, 2021 – The WHO African Region reported 5 Ebola cases, and over 27,000 travelers have been screened in the DRC. Furthermore, over 116 people have been vaccinated.
October 17, 2021 – Africa News reported Ebola vaccinations started in Beni, DRC, after at least two people died due to the virus in October 2021. The WHO African Region Tweeted DRC Situation Report (17/10/21) 5 confirmed cases, three deaths, 369 contacts identified, and 308 contacts monitored.
October 13, 2021 – Democratic Republic of the Congo (DRC) health officials confirmed an Ebola vaccination campaign had launched in the North Kivu province where one confirmed Ebola case, plus three related suspected deaths, were recently reported. About 1,000 doses of the rVSV-ZEBOV Ebola vaccine and other medical supplies were delivered from the capital Kinshasa to Goma city in North Kivu. The DRC has more than 12,000 vaccine doses in Kinshasa that can be deployed if necessary.
October 10, 2021 – The WHO reported additional Ebola cases related to the recent DRC case of a 3-year-old boy. A cluster of three deaths (two children and their father) who were neighbors of the case. These three patients died on 14, 19, and 29 September 2021 after developing symptoms consistent with Ebola. However, none were tested for the virus. As of October 9th, a total of 148 contacts have been identified and are under follow-up by the local response team.
October 8, 2021 – A case of Ebola has been confirmed in the eastern Democratic Republic of the Congo, five months after the end of the most recent Ebola outbreak there. The child died on October 6th. It was not immediately known if the Ebola case was related to the 2018-20 outbreak that killed more than 2,200 people in eastern Congo or the flare-up that killed six people in 2021.
September 13, 2021 – A new study based in Sierra Leone concluded the Ebola vaccine regimen from Janssen – J&J. It was found well tolerated with no safety concerns in children aged 1–17 years and induced robust humoral immune responses, suggesting the suitability of this regimen for Ebola virus disease prevention in children.
August 31, 2021 – The government of Cote d’Ivoire has informed the WHO that a second laboratory has tested samples from a patient suspected of having Ebola and has found no evidence of the virus. Around a dozen WHO experts were mobilized to support the country’s efforts, and 5,000 Ebola vaccine doses which WHO had helped Guinea procure were sent from Guinea to Cote d’Ivoire.
August 23, 2021 – The WHO African region reported Ebola booster dose vaccinations in Sierra Leone following administration of the prime dose of the Johnson & Johnson Ebola vaccine in May 2021. Frontline health workers, practitioners of traditional medicines or traditional healers, and commercial motorbike riders who received the first dose are now given their second jab to maximize their protection against the disease.
August 17, 2021 – The WHO confirmed Cote d’Ivoire deployed 2,000 vaccine doses from Merck and around 3,000 vaccine doses manufactured by Johnson & Johnson – Janssen.
August 14, 2021 – The WHO Africa reported the Ministry of Health of Cote d’Ivoire today confirmed the country’s first case of Ebola since 1994. This came after the Institut Pasteur in Cote d’Ivoire confirmed the Ebola Virus Disease in samples collected from a patient hospitalized in Abidjan’s commercial capital after arriving from Guinea.
August 9, 2021 – The WHO confirmed ‘Marburg virus disease (MVD) is a highly virulent, epidemic-prone disease associated with high case fatality rates (CFR 24-90%). In the early course of the disease, the clinical diagnosis of MVD is difficult to distinguish from other tropical febrile illnesses because of the similarities in the clinical symptoms. Differential diagnoses to be excluded include Ebola virus disease, as well as malaria, typhoid fever, leptospirosis, rickettsial infection, and plague.’
June 15, 2021 – The Southwest National Primate Research Center at Texas Biomedical Research Institute (Texas Biomed) has been awarded more than $37 million from the U.S. National Institutes of Health to continue operations into 2026. The P51 grant, given by the NIH Office of Research Infrastructure Programs, provides essential funding to house and care for nearly 2,500 non-human primates that are part of life-science research programs at Texas Biomed and partners around the globe.
June 4, 2021 – Johnson & Johnson welcomed a new recommendation by the Strategic Advisory Group of Experts on Immunization for the WHO that supports the use of the Johnson & Johnson Ebola vaccine regimen both during outbreaks for individuals at some risk of Ebola exposure and preventively, in the absence of an outbreak, for national and international first responders in neighboring areas or countries where an outbreak might spread.
April 10, 2021 – The government of Sierra Leone and the WHO announced Johnson & Johnson had donated about 4,500 Zabdeno and Mvabea Ebola vaccines to Sierra Leone to help prevent any Ebola outbreak. The last Ebola outbreak in Sierra Leone was in 2016.
March 25, 2021 – Ohio Gov. Mike DeWine revealed health officials are monitoring 44 people who have returned from areas of Africa with active outbreaks of Ebola.
March 25, 2021 – Oregon public health officials announced they are monitoring four people who recently visited the West African countries of Guinea and the Democratic Republic of the Congo. Regions in each of these countries are currently experiencing outbreaks of Ebola virus disease. The Oregon Health Authority and local public health departments have been in contact with these individuals, considered “persons under monitoring” since they arrived in the state earlier in March 2021.
March 23, 2021 – The WHO African Region Tweeted Guinea Ebola outbreak Situation Report (22/03/21) 18 cases, nine deaths, 78 contacts, 82% monitored. And 3,905 people have been vaccinated.
March 13, 2021 – After a request from the Guinean authorities, Russia is considering supplying a domestic vaccine against the Ebola virus to the African country, reported TASS.
May 13, 2020 – BARDA Provides the Sabin Vaccine Institute with an Additional $20 Million for Further Development of Ebola Sudan and Marburg Vaccines
The Sabin Vaccine Institute (Sabin) and its partner ReiThera Srl today announced that the Biomedical Advanced Research and Development Authority (BARDA), part of the Office of the Assistant Secretary for Preparedness and Response within the U.S. Department of Health and Human Services, has exercised the first two options, valued at $20 million, under the 2019 contract to advance the development of vaccines against Ebola Sudan and Marburg viruses through Phase 2 clinical trials. In September 2019, BARDA awarded Sabin a development contract, valued at $128 million, and provided the initial funding award of $20.5 million. This second $20 million award will enable the manufacture and release of clinical vaccine material developed by ReiThera, a specialist in the development and cGMP manufacture of adenoviral vector vaccines. The funding will also support non-clinical studies to evaluate efficacy and immune response.
UPDATE 5: NOVEMBER 7, 2021: MARBURG GOES VIRAL ON INTERNET ONLY, YET. I’m happy awareness increases, it’s crucial. I’ve addressed this virus below, but not many had the patience to go through all text, and I kind of understand them, but there’s no easier way than reading. Here’s another angle to keep in sight when computing all this info:
UPDATE 4: OCTOBER 19 2021: THE FEARPORN CAMPAIGN TAKES SPEED AS IF THEY ARE TO RELEASE THIS SOON. IF YOU FALL FOR THEIR BRAINWASH, THEY HAVE NO REASON TO STOP.
And they’re still not running out of stupid ideas we can see through:
Oh, look who pushes the fear! Exactly who I would’ve expected:
Later update: In the meantime I’ve learned that Marburg (an Ebola relative) and Xinjiang fever, a Chinese relative of the Yellow Fever virus, are also top candidates, and that goes in line with the Fauci e-mails I highlighted below. I will be back with more details shortly. Almost certainly it will be some form of hemorrhagic fever, most likely to cover for injections side-effects on the blood stream.
UPDATE 2:
One month later, they’re starting to catch up and it’s still not too late to un-play it if this goes BOOM NOW!
By the end of last century, The Military has abandoned you and has joined Pharmafia and the super-rich elites in a plan to govern you with bioweapons and psy-ops. As I’ve said many times, Big Pharma and Big Tech are long gone, The Military BioTech Complex has been running the show for quite a while. This is just a chapter from that book, more to come if we get some love.
Canadian lab’s shipment of Ebola, Henipah viruses to China raises questions
Henipah and Nipah are interchangeable
Scientists at the National Microbiology Lab sent live Ebola and Henipah viruses to Beijing on an Air Canada flight March 31, and while the Public Health Agency of Canada says all federal policies were followed, there are questions about whether that shipment is part of an ongoing RCMP investigation.
Ebola and Henipah are Level 4 pathogens, meaning they’re some of the deadliest viruses in the world. They must be contained in a lab with the highest level of biosafety control, such as the one in Winnipeg.
Two months after that shipment, on May 24, the Public Health Agency of Canada (PHAC) referred an “administrative matter” to RCMP that resulted in the removal of two Chinese research scientists — Xiangguo Qiu and Keding Cheng — and several international students on July 5.
Both agencies have said repeatedly that public safety has not been at risk.
PHAC will not confirm if the March 31 shipment is part of the RCMP investigation.
Strict protocols
Several sources, who have asked to remain anonymous because they fear for their jobs, say the pathogens may have been shipped to the Chinese Academy of Sciences in a way that circumvented the lab’s operating procedures, and without a document protecting Canada’s intellectual property rights.
Researchers working at the National Microbiology Lab on cutting-edge, high-containment research are not allowed to send anything to other countries or labs without the intellectual property office negotiating and having a material transfer agreement in place, in case the material sent leads to a notable discovery.
A PHAC spokesperson did not confirm if this shipment included such an agreement.
However, Eric Morrissette said it’s “routine” for the lab to share samples of pathogens and toxins with partners in other countries to advance scientific work worldwide.
“All transfers of Risk Group 4 samples follow strict transportation requirements and are authorized by senior officials at the lab and the NML tracks and keeps electronic records of all shipments of samples in accordance with the HPTA. Agreements for the transfer of materials are determined on a case-by-case basis,” Morrisette wrote in an email statement.
“On the specific shipments to China earlier this year, we can confirm that we have all records pertaining to the shipment, and that all protocols were followed as directed by the above Acts and Standards.”
Xiangguo Qiu is head of the National Microbiology Lab’s Vaccine Development and Antiviral Therapies section in the Special Pathogens Program. She is responsible for the lab that works with Ebola. Her husband, Keding Cheng, is also a PHAC biologist.
After their security clearance was revoked and they were escorted from the lab, the University of Manitoba also cut ties with them and re-assigned Qiu’s graduate students, pending the RCMP investigation. No charges have been laid.
Neither scientist has responded to requests for comment, although some of their former colleagues say Qiu is not just a world-renowned scientist who helped develop a treatment for Ebola, but also a researcher with ethics and integrity.
Case raises questions
One question raised by this case is that of intellectual property protection, says Leah West, who practises, studies and publishes in the field of national security law and lectures at the Norman Paterson School of International Affairs.
“If China was leveraging these scientists in Canada to gain access to a potentially valuable pathogen or to elements of a virus without having to license the patent … it makes sense with the idea of China trying to gain access to valuable IP without paying for it,” she said.
West accepts PHAC’s assertion that public safety is not an issue, even though the viruses were transported on a commercial Air Canada flight.
However, she says the fact the RCMP is involved means there’s a legitimate concern.
“You don’t send a policy breach, a bureaucratic policy breach, to the RCMP to investigate unless you believe that that policy breach has resulted in a criminal offence or could have resulted in a criminal offence. So what is the criminal offence potentially here?” West said.
She said she hopes the lab and Health Canada are also doing an internal investigation.
“I think there will need to be an inquiry into the scientists to potentially see whether or not they were compromised or any elements of their work were compromised and that China gained illegal or improper access to Canadian intellectual property … to see what China may have gained access to without knowledge, prior to this incident,” West says.
Don’t ‘jump into any conclusions too quickly’
However, the deputy director of the University of Alberta’s China Institute is urging caution when it comes to making assumptions.
Jia Wang doesn’t dispute China has been involved in the past in espionage and intellectual property theft, but she says that country is making big investments in developing STEM (science, technology, engineering and mathematics) scholars and then putting that into innovation.
China has its own reasons to protect intellectual property because many new ideas are coming from there, Wang says.
She’s waiting to see what comes of the RCMP investigation of the lab in Winnipeg.
“As China observers, we’d like to perhaps gently remind people not to jump into any conclusions too quickly,” she said.
“It will be good to get to the bottom of this and see what might have gone wrong and what was the oversight and how can the procedures be improved or people involved can be reminded of how to adhere to the policies better.”
The shipment of the viruses took place at a time when relations between Canada and China have been strained over the arrest of a Huawei executive, at the request of the United States.
In retaliation, China has detained two Canadians and is boycotting Canadian canola and pork.
Because of the strained relationship between the two countries, and this case at the lab, Chinese-Canadian researchers and academics are starting to worry they may be singled out and targeted, Wang said.
“Certain assumptions are made or their loyalty to Canada is questioned in any way. And as multicultural as we are in Canada, we don’t want to see that.” – CBC, 2019
On December 19, 2019, the U.S. Food and Drug Administration announced the approval of Ervebo to prevent EVD caused by Zaire ebolavirus in individuals 18 years of age and older. This report, published by the U.S. CDC on January 8, 2021, summarizes the Advisory Committee on Immunization Practices (ACIP) recommendations for using the rVSVΔG-ZEBOV-GP Ebola vaccine (Ervebo) in the USA.
On July 1, 2020, the European Medicines Agency granted Johnson & Johnson Janssen’s Zabdeno and Mvabea Ebola vaccine therapy, a prime-boost vaccination approach for preventing infectious diseases. Janssen’s Ebola vaccine regimen is specifically designed to induce long-term immunity against the Ebola virus in adults and children aged one year and above.
CanSino Biologics’s Ad5-EBOV Ebola vaccine received approval in China in October 2017. Ad5-EBOV is an adenovirus type 5 vector-based Ebola virus disease vaccine that protects against Ebola by relying on the recombinant replication-defective human adenovirus type-5 vector immune response. In addition, Ad5-EBOV is manufactured as a lyophilized powder, highly stable, and does not require storage at ultra-low temperatures. This feature renders it viable for use in resource-limited tropical areas.
The WHO published the revised Ebola Vaccine FAQ on January 11, 2020.
Henipaviruses belong to the family of paramyxoviruses. Two species have been identified to be zoonotic, causing disease in animals. These are the Hendra virus (HeV) and the Nipah virus (NiV). They produce severe and often fatal illness in humans and horses.
Samples from early Wuhan COVID-19 patients show the presence of genetically modified Henipah virus, an American scientist has found.
Henipah was one of the two types of viruses sent to China by Chinese-born scientists from a Canadian laboratory at the centre of a controversy over the firing of the scientists and collaboration with Chinese military researchers. It is not clear whether the virus found in the Chinese samples is related to the samples sent by the Canadian lab, which were shipped in late March 2019.
The finding was confirmed for The Epoch Times by another qualified scientist.
The evidence was first found by Dr. Steven Quay, a Seattle-based physician-scientist and former faculty member at the Stanford University School of Medicine, who looked at early COVID-19 samples uploaded by scientists at the Wuhan Institute of Virology (WIV) shortly after China informed the World Health Organization about the SARS-CoV-2 outbreak.
Chinese virologist Shi Zhengli is seen inside the P4 laboratory in Wuhan, China, on Feb. 23, 2017. (Johannes Eisele/AFP via Getty Images)
The samples from the patients, who reportedly were found to have the “unknown pneumonia” in December 2019, were uploaded to the genetic sequence database, GenBank, on the website of the U.S. National Institute of Health (NIH).
Quay says that while other scientists around the world were mostly interested in examining the genome of SARS-CoV-2 in the samples uploaded by the WIV scientists, he wanted to see what else was in the samples collected from the patients.
So he collaborated with a few other scientists to analyze sequences from the samples.
“We started fishing inside for weird things,” Quay told The Epoch Times.
What they found, he says, are the results of what could likely be contamination from different experiments in the lab making their way into the samples, as well as evidence of Henipah virus.
“We found genetic manipulation of the Nipah virus, which is more lethal than Ebola.” Nipah is a type of Henipah virus.
The Epoch Times asked Joe Wang, PhD, who formerly spearheaded a vaccine development program for SARS in Canada with one of the world’s leading pharmaceutical companies, to verify the finding. Wang is currently the president of NTD Television Canada, the sister company of The Epoch Times in Canada.
After examining the evidence, Wang said he was able to replicate Quay’s findings on the Henipah virus. He explains that the genetic manipulation of the virus was likely for the purposes of vaccine development.
Winnipeg Lab
The firing of Chinese-born scientist Xiangguo Qiu and her husband, Keding Cheng, from the National Microbiology laboratory (NML) in Winnipeg has been the subject of much controversy in Canada, with opposition parties pressing the government for more details on the case, and the government refusing to release information citing national security and privacy concerns.
Qiu and Cheng along with several Chinese students were escorted out of NML, Canada’s only Level 4 lab, in July 2019, amid a police investigation. The two scientists were formally fired in January 2021.
The Public Health Agency of Canada (PHAC), which is in charge of NML, said the termination was the result of an “administrative matter” and “possible breaches of security protocols,” but has declined to provide further details, citing security and privacy concerns.
House Speaker Anthony Rota admonishes Public Health Agency of Canada President Iain Stewart in the House of Commons on June 21, 2021, for failing to provide documents related to the firing of two scientists from the National Microbiology Laboratory in Winnipeg. (The Canadian Press/Sean Kilpatrick)
During her time at NML, Qiu travelled several times in an official capacity to WIV, helping train personnel on Level 4 safety. The Globe and Mail later reported that scientists at NML have been collaborating with Chinese military researchers on deadly pathogens, and that one of the Chinese military researchers worked at the high-security Winnipeg lab for a period of time.
Documents and emails released by PHAC show that the shipment of Henipah and Ebola samples was done with the permission of NML authorities.
In one of the emails sent in September 2018, David Safronetz, chief of special pathogens at PHAC, informs then-head of NML Matthew Gilmour and other lab administrators about the request from WIV for the shipment of the samples, saying “I trust the lab.”
In response, Gilmour asks about the nature of the work that will be done at the Wuhan lab, and why the lab doesn’t get the material from “other, more local labs.” He also tells Safronetz that it’s “good to know that you trust this group,” asking how NML was connected with them.
In his reply, Safronetz doesn’t specifically say what the samples will be used for in China, but notes they will only be sent once all paperwork and certification is completed. He also says the WIV is requesting the material from NML “due to collaboration” with Qiu.
He adds, “Historically, it’s also been easier to obtain material from us as opposed to US labs. I don’t think other, closer labs have the ability to ship these materials.”
Gilmour resigned from his position at NML in May 2020 and joined a UK-based bioresearch company.
MPs have asked NML management why shipment of the samples was allowed and whether they knew if China performs any Gain of Function (GoF) research at WIV. GoF research involves increasing the lethal level (virulence) or transmissibility of pathogens.
NML’s acting scientific director general Guillaume Poliquin told MPs during a parliamentary committee meeting on March 22 that the lab only sent the samples to WIV after receiving assurance that no GoF research would take place.
Conservative MP John Williamson pressed for more answers, saying the word of the state-run Chinese lab can’t be trusted as the Chinese regime “has a history of theft and lies.”
The issue of GoF research at WIV has been a point of contention in the United States between lawmakers and Dr. Anthony Fauci, NIH’s head of the National Institute of Allergy and Infectious Diseases, whose organization has funded research (through EcoHealth Alliance) on coronaviruses at the Wuhan lab. U.S. Sen. Rand Paul says published work from WIV on coronaviruses shows the lab is conducting GoF research, a charge Fauci denies.
The P4 laboratory on the campus of the Wuhan Institute of Virology in Wuhan, China, on May 13, 2020. (Hector Retamal/AFP via Getty Images)
The Epoch Times sought comment from PHAC, including as to how the agency addressed issues of intellectual property and the development of any products such as vaccines with WIV, but didn’t hear back by time of publication.
Despite repeated requests by opposition parties for more details related to the firing of the two NML scientists, the Liberal government has refused to provide records, saying there are national security and privacy concerns.
After the House of Commons issued an order for the government to disclose the information, the government took the Speaker of the House to court to obtain confirmation from a judge that it can withhold the documents. The government later dropped its court case once Prime Minister Justin Trudeau called an election and Parliament was dissolved. – Epoch Times
UPDATE 3: I FOUND CREDIBLE SOURCES FOR MOST OF DR. ARYANA LOVE’S EXPLOSIVE CLAIMS BELOW:
I didn’t have an in depth look at all her sources, I can’t have a final 100% verdict, but I did more than a glance and no lies detected. You can review her blog post yourself HERE. This might be the closure to this report and the start for another.
OBAMA: EBOLA RESPONSE A TRIAL RUN FOR A POTENTIAL AIRBORNE VIRUS THAT MIGHT HIT SOON (2014)
BONUS
This is from 2014, but the story goes a way long back. And forward. Let’s not forget Putin is a Davos regular since before he became such a literal czar.
WHERE IT’S AT EXACTLY TWO YEARS LATER (SEPT. 2023)
meanwhile, we found out that…
In March 2015, a CureVac investor, the Bill & Melinda Gates Foundation, agreed to provide separate funding for several projects to develop prophylactic vaccines based on CureVac’s proprietary mRNA platform… n July 2020, Tesla, Inc CEO Elon Musk announced via Tweet that Tesla and CureVac had reached an agreement to produce portable “RNA microfactories” based on this technology to manufacture CureVac’s COVID-19 vaccine candidate. CureVac had stated that the bioprinters would be able to produce “more than a hundred thousand doses” within approximately two weeks. At approximately the same time, Tesla and CureVac filed a joint patent on the technology. In August, Musk reviewed the project with Curevac while in Germany.
How much of the tsunami is fabricated in Musk’s factories?
So we’re back at:
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them









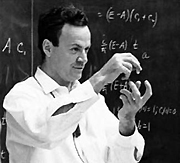
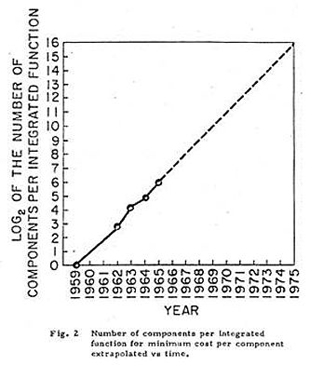
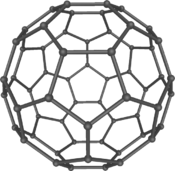
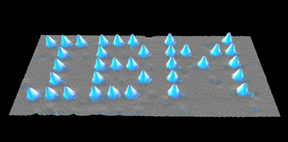
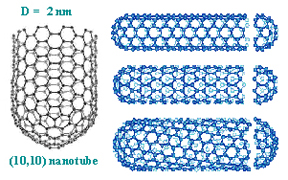
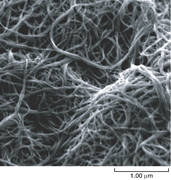
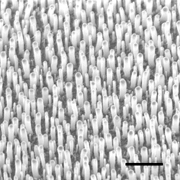
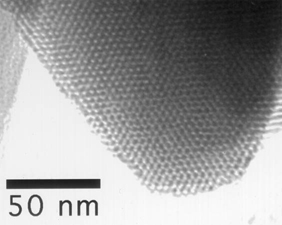
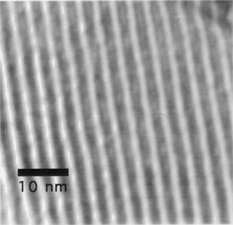
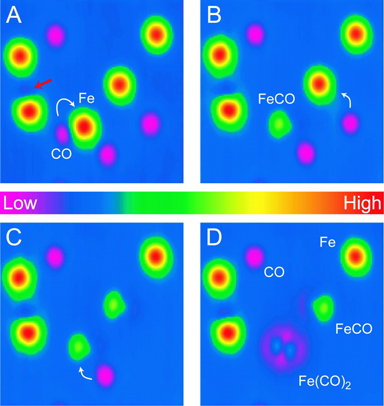
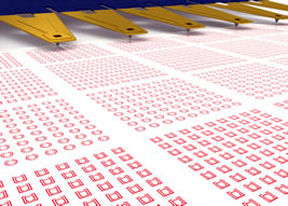

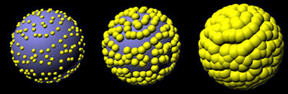
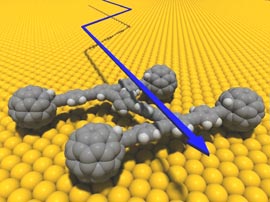
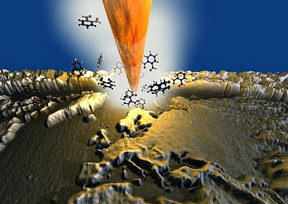




































































































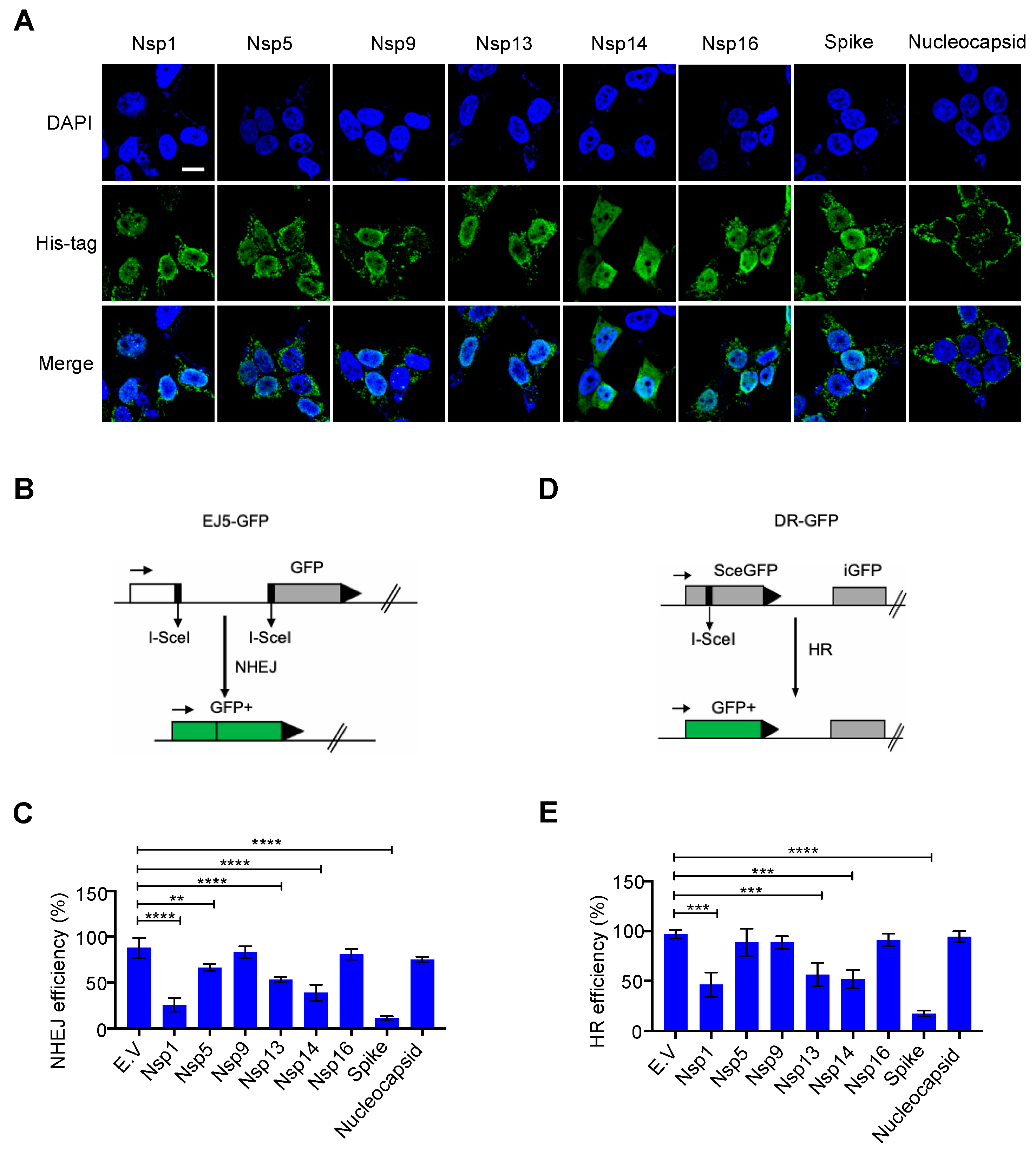{kind=link}
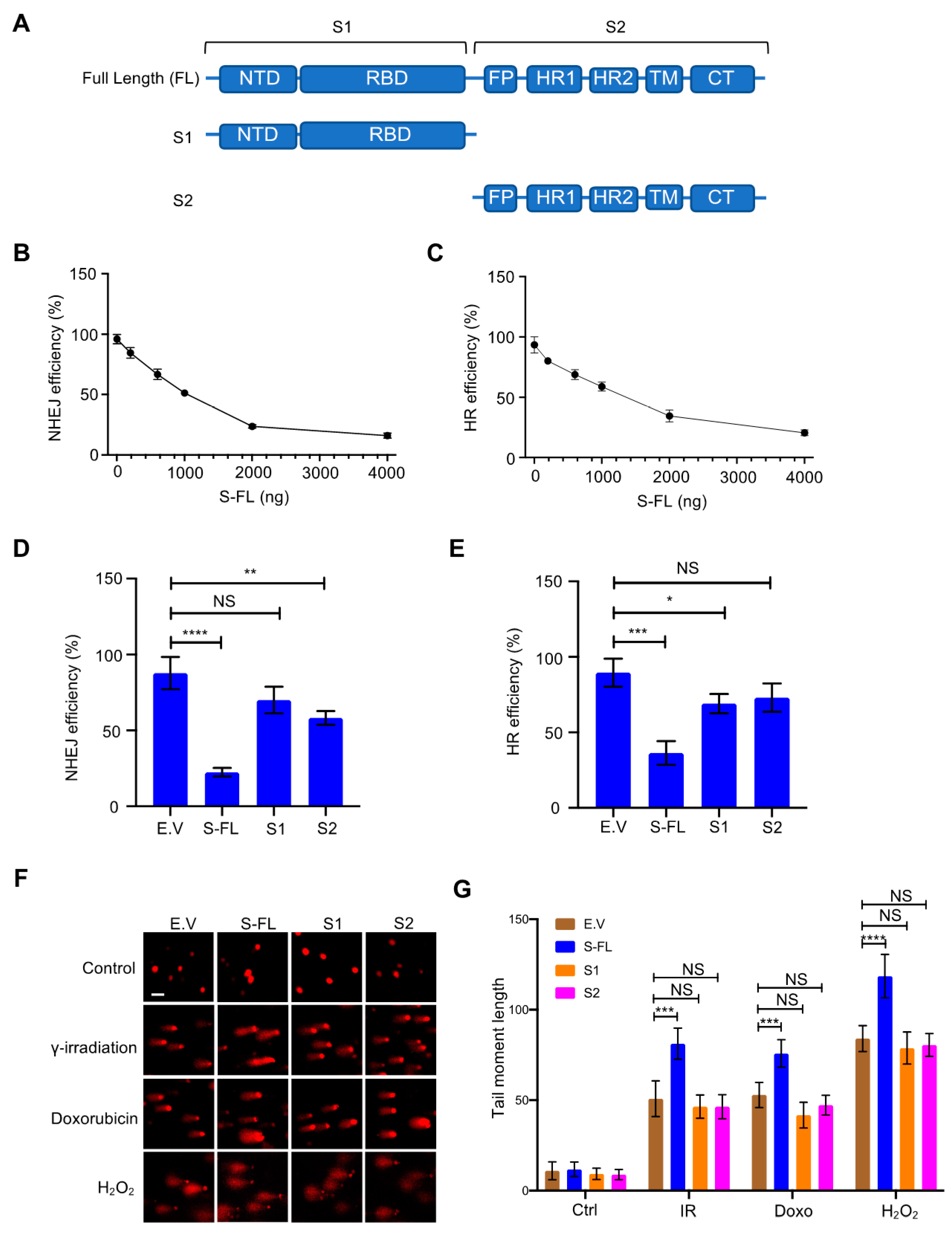{kind=link}
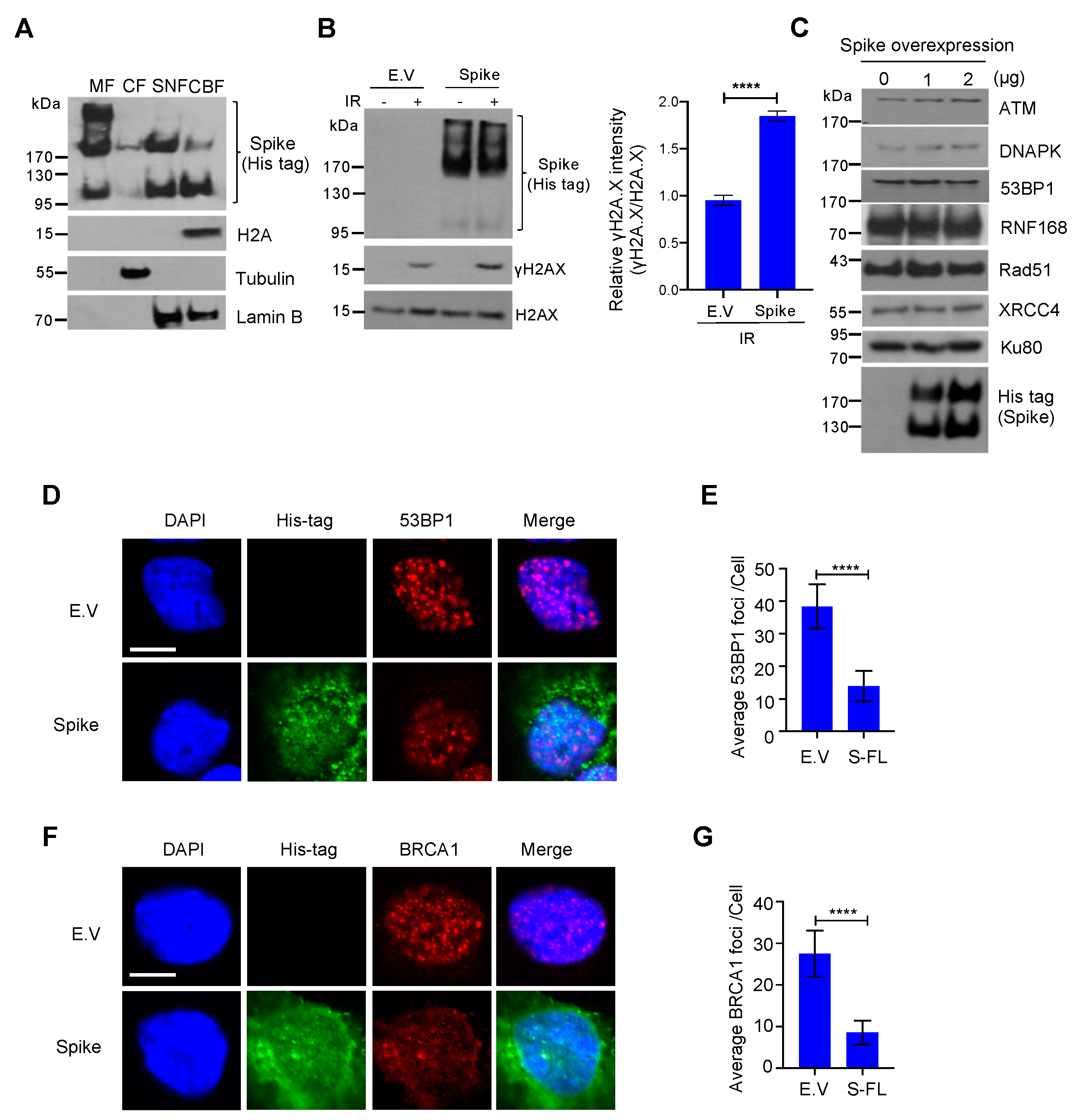{kind=link}
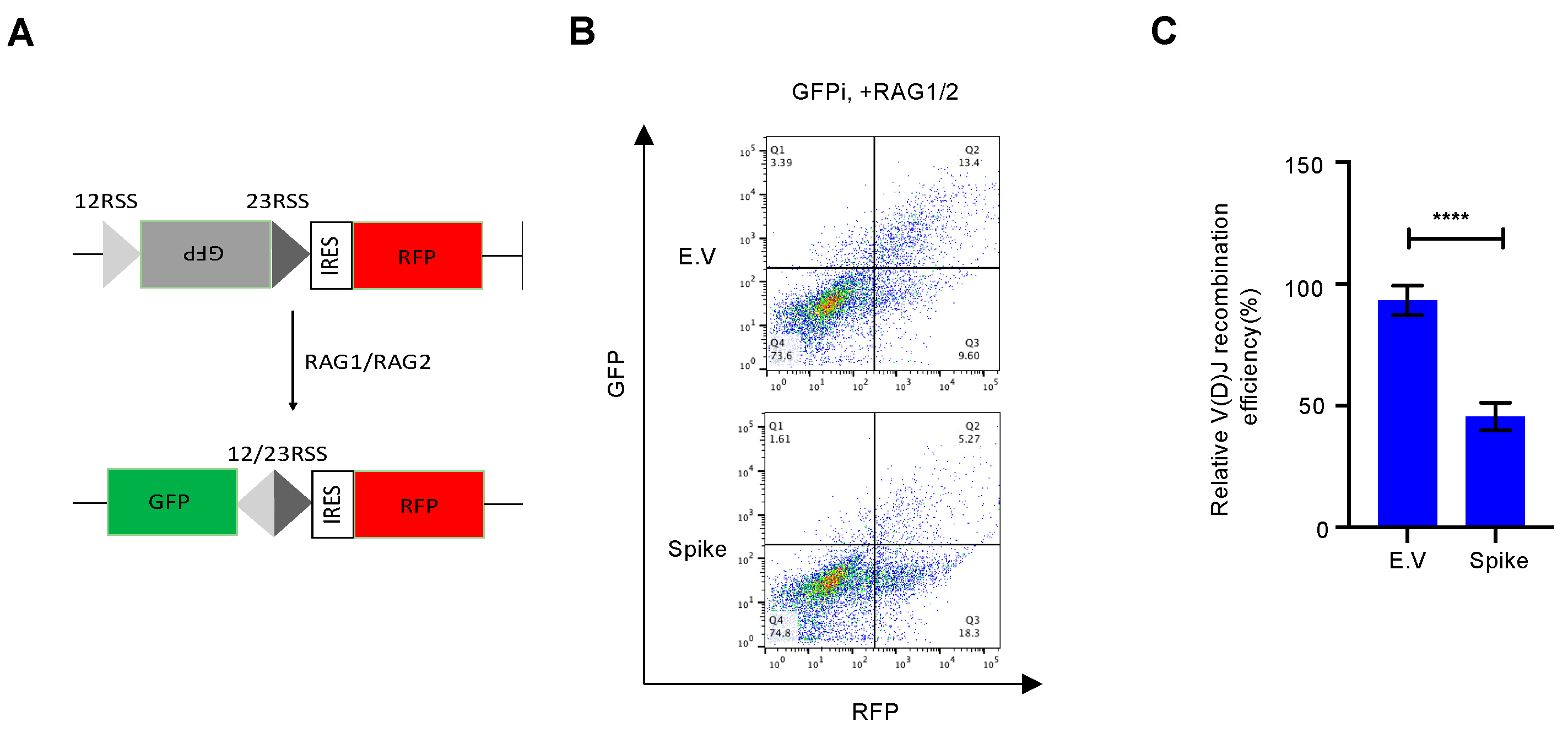{kind=link}